

Pulmonary Artery Pressure-Guided Heart Failure Management Reduces Hospitalizations in Patients With Chronic Kidney Disease
- PMID: 37192290
- PMCID: PMC10179985
- DOI: 10.1161/CIRCHEARTFAILURE.122.009721
Pulmonary Artery Pressure-Guided Heart Failure Management Reduces Hospitalizations in Patients With Chronic Kidney Disease
Erratum in
-
Correction to: Pulmonary Artery Pressure-Guided Heart Failure Management Reduces Hospitalizations in Patients With Chronic Kidney Disease.Circ Heart Fail. 2023 Aug;16(8):e000081. doi: 10.1161/HHF.0000000000000081. Epub 2023 Aug 15. Circ Heart Fail. 2023. PMID: 37582167 Free PMC article. No abstract available.
Abstract
Background: Hemodynamic-guided heart failure management is a superior strategy to prevent decompensation leading to hospitalization compared with traditional clinical methods. It remains unstudied if hemodynamic-guided care is effective across severities of comorbid renal insufficiency or if this strategy impacts renal function over time.
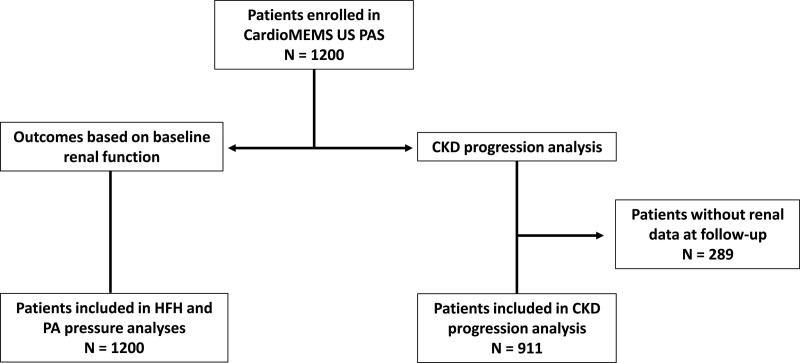
Methods: In the CardioMEMS US PAS (Post-Approval Study), heart failure hospitalizations were compared from 1 year before and after pulmonary artery sensor implantation in 1200 patients with New York Heart Association class III symptoms and a previous hospitalization. Hospitalization rates were evaluated in all patients grouped into baseline estimated glomerular filtration rate (eGFR) quartiles. Chronic kidney disease progression was evaluated in patients with renal function follow-up data (n=911).
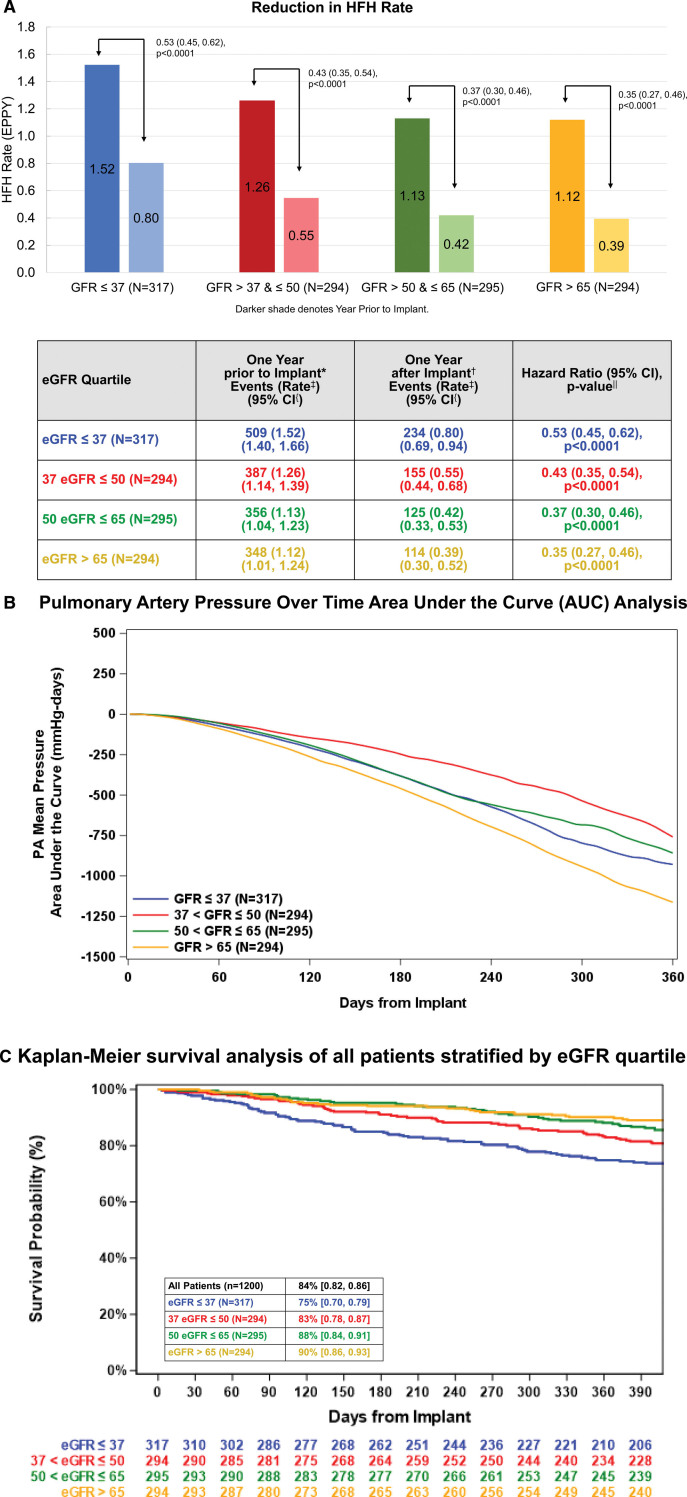
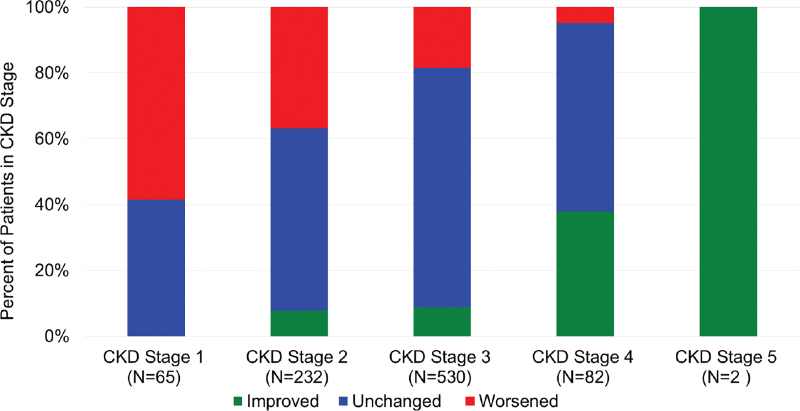
Results: Patients with stage 2 or greater chronic kidney disease at baseline exceeded 80%. Heart failure hospitalization risk was lower in all eGFR quartiles ranging from a hazard ratio of 0.35 (0.27-0.46; P<0.0001) in patients with eGFR >65 mL/min per 1.73 m2 to 0.53 (0.45-0.62; P<0.0001) in patients with eGFR ≤37 mL/min per 1.73 m2. Renal function was preserved or improved in most patients. Survival was different between quartiles and lower in quartiles with more advanced chronic kidney disease.
Conclusions: Hemodynamic-guided heart failure management using remotely obtained pulmonary artery pressures is associated with lower hospitalization rates and general preservation of renal function in all eGFR quartiles or chronic kidney disease stages.
Keywords: diuretics; heart failure; hemodynamics; hospitalization; renal insufficiency.
Conflict of interest statement
Figures
References
-
- Heywood JT, Fonarow GC, Costanzo MR, Mathur VS, Wigneswaran JR, Wynne J; ADHERE Scientific Advisory Committee and Investigators. High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heart failure: a report from the ADHERE database. J Card Fail. 2007;13:422–430. doi: 10.1016/j.cardfail.2007.03.011 - PubMed
-
- Herzog CA, Muster HA, Li S, Collins AJ. Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the medicare population. J Card Fail. 2004;10:467–472. doi: 10.1016/j.cardfail.2004.03.003 - PubMed
-
- Ong MK, Romano PS, Edgington S, Aronow HU, Auerbach AD, Black JT, Marco T, Escarce JJ, Evangelista LS, Hanna B, et al. . Effectiveness of remote patient monitoring after discharge of hospitalized patients with heart failure: the Better Effectiveness After Transition -- Heart Failure (BEAT-HF) randomized clinical trial. JAMA Internal Medicine. 2016;176:310–318. doi: 10.1001/jamainternmed.2015.7712 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
