

A phase 3, randomised, double-blind, placebo-controlled clinical trial evaluation of the efficacy and safety of a SARS-CoV-2 recombinant spike RBD protein vaccine in adults (ABDALA-3 study)
- PMID: 37192953
- PMCID: PMC10160525
- DOI: 10.1016/j.lana.2023.100497
A phase 3, randomised, double-blind, placebo-controlled clinical trial evaluation of the efficacy and safety of a SARS-CoV-2 recombinant spike RBD protein vaccine in adults (ABDALA-3 study)
Abstract
Background: The pandemic of COVID-19 raised the urgent need for safe and efficacious vaccines against SARS-CoV-2. We evaluated the efficacy and safety of a new SARS-CoV-2 virus receptor-binding domain (RBD) vaccine.
Methods: A phase 3, multicentre, randomised, double-blind, placebo-controlled trial was carried out at 18 clinical sites in three provinces of the south-eastern region of Cuba. Subjects (healthy or those with controlled chronic diseases) aged between 19 and 80 years, who gave written informed consent were eligible. Subjects were randomly assigned (1:1, in blocks) to two groups: placebo, and 50 μg RBD vaccine (Abdala). The product was administered intramuscularly, 0.5 mL in the deltoid region, in a three-dose immunization schedule at 0-14-28 days. The organoleptic characteristics and presentations of the vaccine and placebo were identical. All participants (subjects, clinical researchers, statisticians, laboratory technicians, and monitors) remained blinded during the study period. The main endpoint was to evaluate the efficacy of the Abdala vaccine in the prevention of symptomatic COVID-19. The trial is registered with the Cuban Public Registry of Clinical Trials, RPCEC00000359.
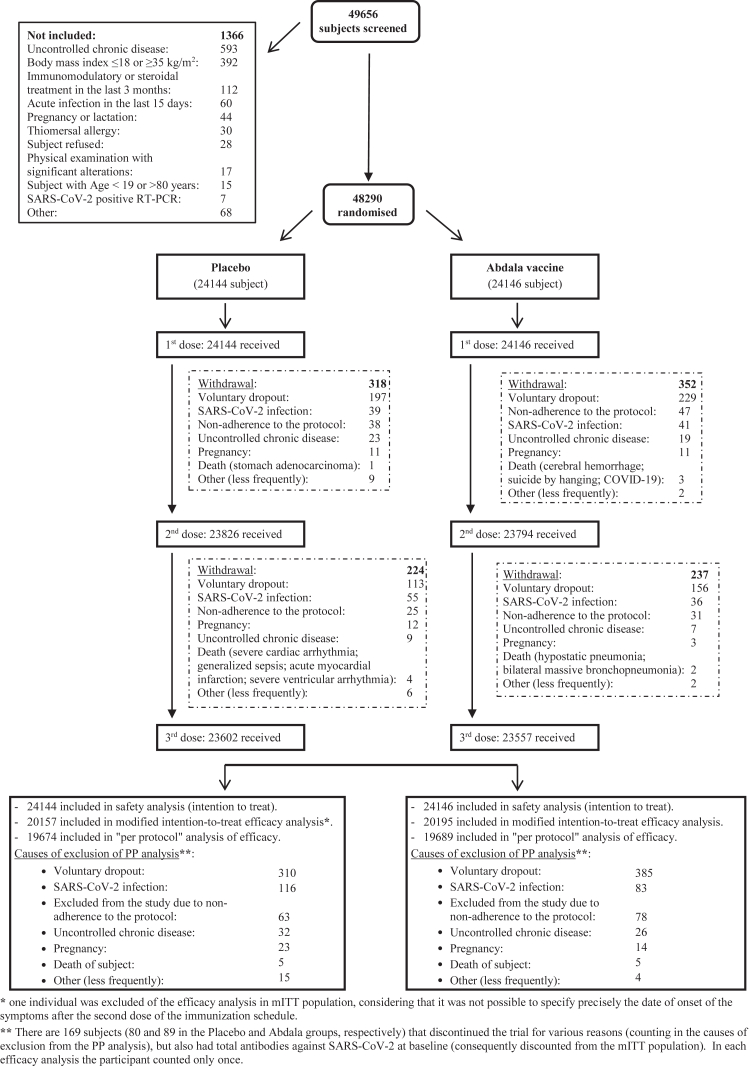
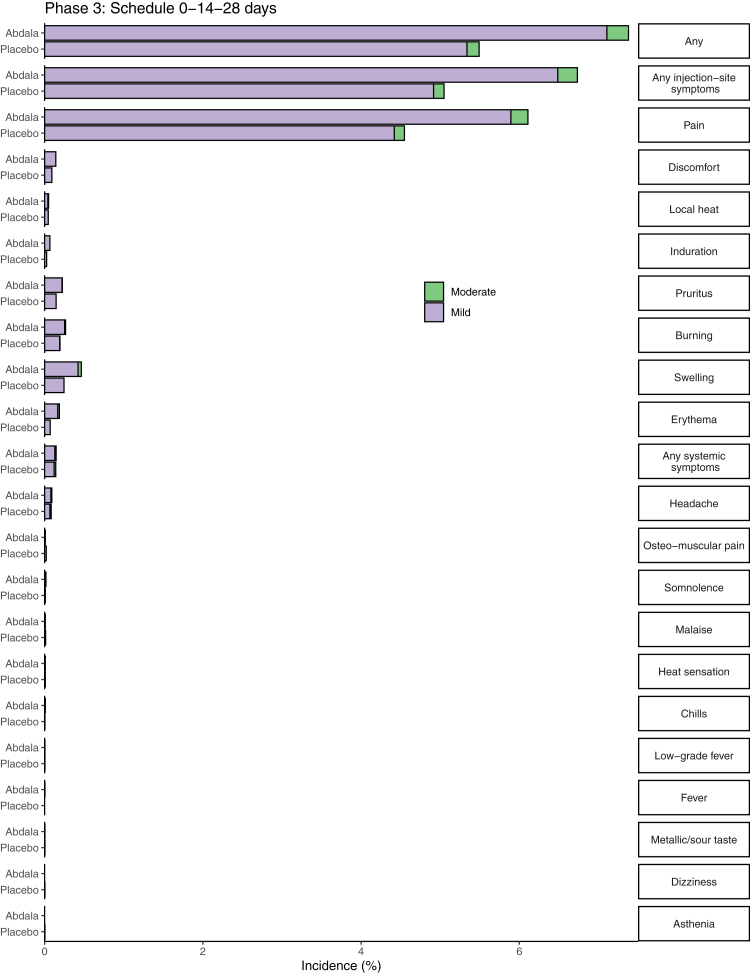
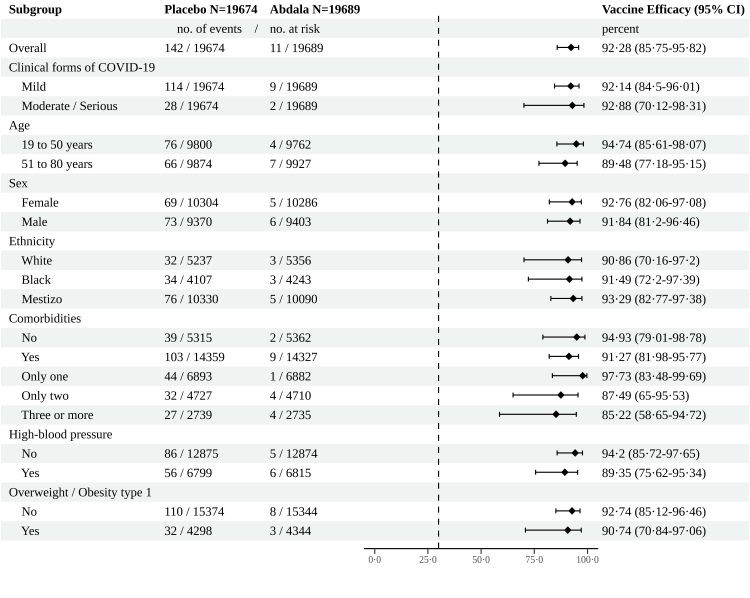
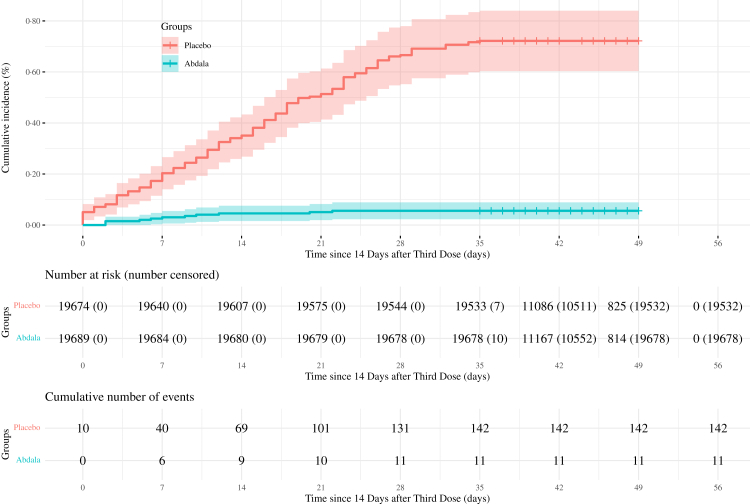
Findings: Between March 22 to April 03, 2021, 48,290 subjects were included (24,144 and 24,146 in the placebo and Abdala groups, respectively) in the context of predominant D614G variant circulation. The evaluation of the main efficacy outcomes occurred during May-June 2021, starting at May 3rd, in the context of high circulation of mutant viruses, predominantly VOC Beta. The incidence of adverse reactions for individuals in the placebo and Abdala vaccine groups were 1227/24,144 (5.1%) and 1621/24,146 (6.7%), respectively. Adverse reactions were mostly mild, and from the injection site, which resolved in the first 24-48 h. No severe adverse events with demonstrated cause-effect relationship attributable to the vaccine were reported. Symptomatic COVID-19 disease was confirmed in 142 participants in the placebo group (78.44 incidence per 1000 person-years, 95% confidence interval [CI], 66.07-92.46) and in 11 participants in Abdala vaccine group (6.05 incidence per 1000 person years; 95% CI 3.02-10.82). The Abdala vaccine efficacy against symptomatic COVID-19 was 92.28% (95% CI 85.74-95.82). Moderate/serious forms of COVID-19 occurred in 30 participants (28 in the placebo group and only 2 in the Abdala vaccine group) for a vaccine efficacy of 92.88% (95% CI 70.12-98.31). There were five critical patients (of which four died), all in the placebo group.
Interpretation: The Abdala vaccine was safe, well tolerated, and highly effective, fulfilling the WHO target product profile for COVID-19 vaccines. Those results, along with its immunization schedule and the advantage of easy storage and handling conditions at 2-8 °C, make this vaccine an option for the use in immunization strategies as a key tool for the control of the pandemic.
Funding: Centre for Genetic Engineering and Biotechnology (CIGB), Havana, Cuba.
Keywords: COVID-19; Controlled clinical trial; Double-blind; Efficacy; Phase 3; Placebo-controlled clinical trial; Randomised; SARS-CoV-2; Spike RBD protein; Vaccine.
© 2023 The Author(s).
Conflict of interest statement
FHB, YMB, KlUP, KaUP, JQG, JLRR, IBC, GMS, MLF, MAV, RHR, KMCA, MAA, and VLMG, are employees at the Genetic Engineering and Biotechnology Centre, Havana Network, where Abdala vaccine active ingredient is produced and the formulation was developed. The remaining authors have no conflict of interest. No honoraria, consulting fees or payments for seminar presentations, speeches or appearances have been received by any of the authors.
Figures
References
-
- World Health Organization Weekly epidemiological update on COVID-19-24 August 2022. 2022. https://www.who.int/publications/m/item/weekly-epidemiological-update-on... Available at:
-
- Centers for Disease Control and Prevention COVID-19 risks and vaccine information for older adults. https://espanol.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/old... Available at:
-
- Izquierdo M., Ramos Y., Costa L., et al. Demonstrating “Abdala” subunit vaccine thermostability. BioProcess J. 2022;21 doi: 10.12665/J21OA.Izquierdo. - DOI
-
- Hernández-Bernal F., Ricardo-Cobas M.C., Martin-Bauta Y., et al. Safety, tolerability, and immunogenicity of a SARS-CoV-2 recombinant spike RBD protein vaccine: a randomised, double-blind, placebo-controlled, phase 1-2 clinical trial (ABDALA Study) eClinicalMedicine. 2022;101383:46. doi: 10.1016/j.eclinm.2022.101383. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
