

Probable trauma associated sleep disorder in post-9/11 US Veterans
- PMID: 37193287
- PMCID: PMC10108646
- DOI: 10.1093/sleepadvances/zpad001
Probable trauma associated sleep disorder in post-9/11 US Veterans
Abstract
Study objectives: The purpose of this study was to (1) estimate trauma associated sleep disorder (TASD) prevalence among post-9/11 era veterans and to describe differences in service and comorbid mental health clinical characteristics among individuals with and without probable TASD, and (2) estimate TASD prevalence and characteristics of reported traumatic experiences stratified by sex.
Methods: We used cross-sectional data from the post-deployment mental health study of post-9/11 veterans, which enrolled and collected baseline data from 2005 to 2018. We classified veterans as having probable TASD using self-reported measures: traumatic experiences from the traumatic life events questionnaire (TLEQ) and items from the Pittsburgh sleep quality index with Addendum for posttraumatic stress disorder (PTSD) mapped to TASD diagnostic criteria and ascertained mental health diagnoses (PTSD, major depressive disorder [MDD]) via Structured Clinical Interview for DSM-IV. We calculated effect sizes as prevalence ratios (PR) for categorical variables and Hedges' g for continuous variables.
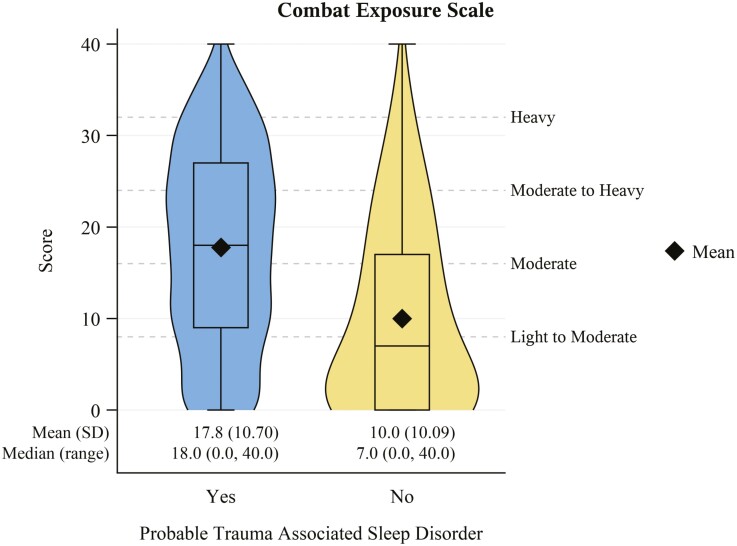
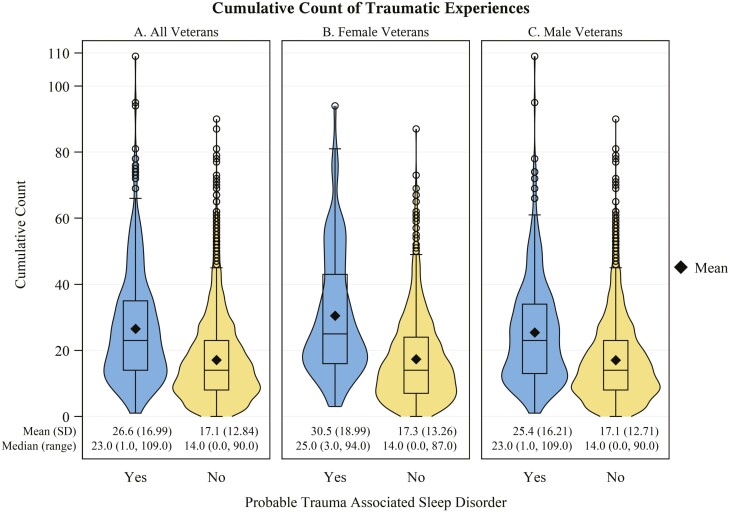
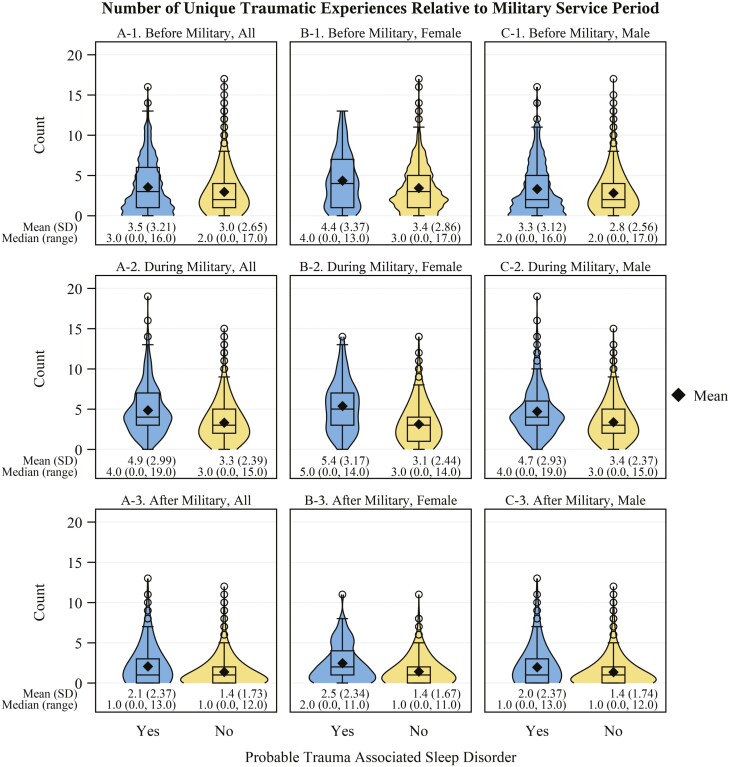
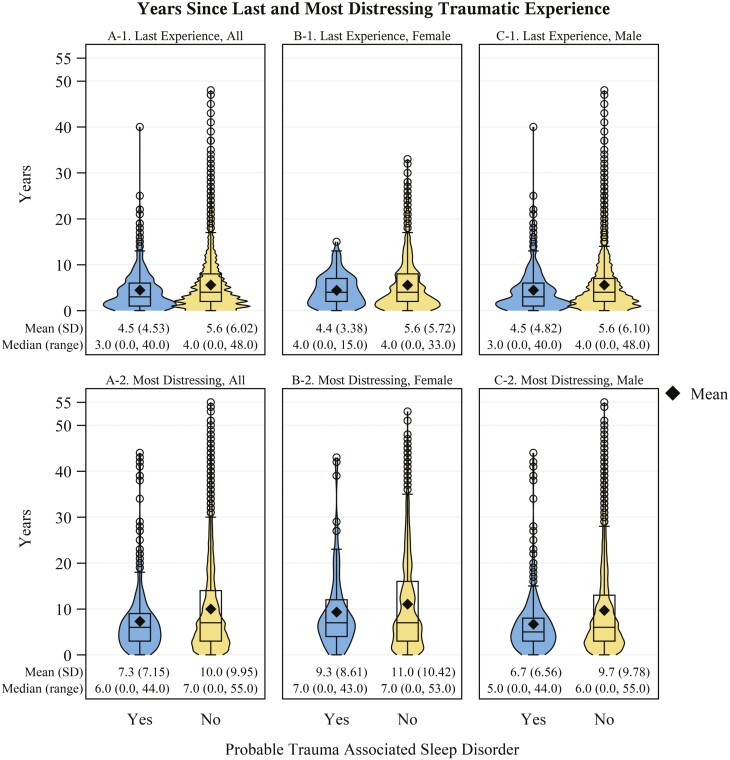
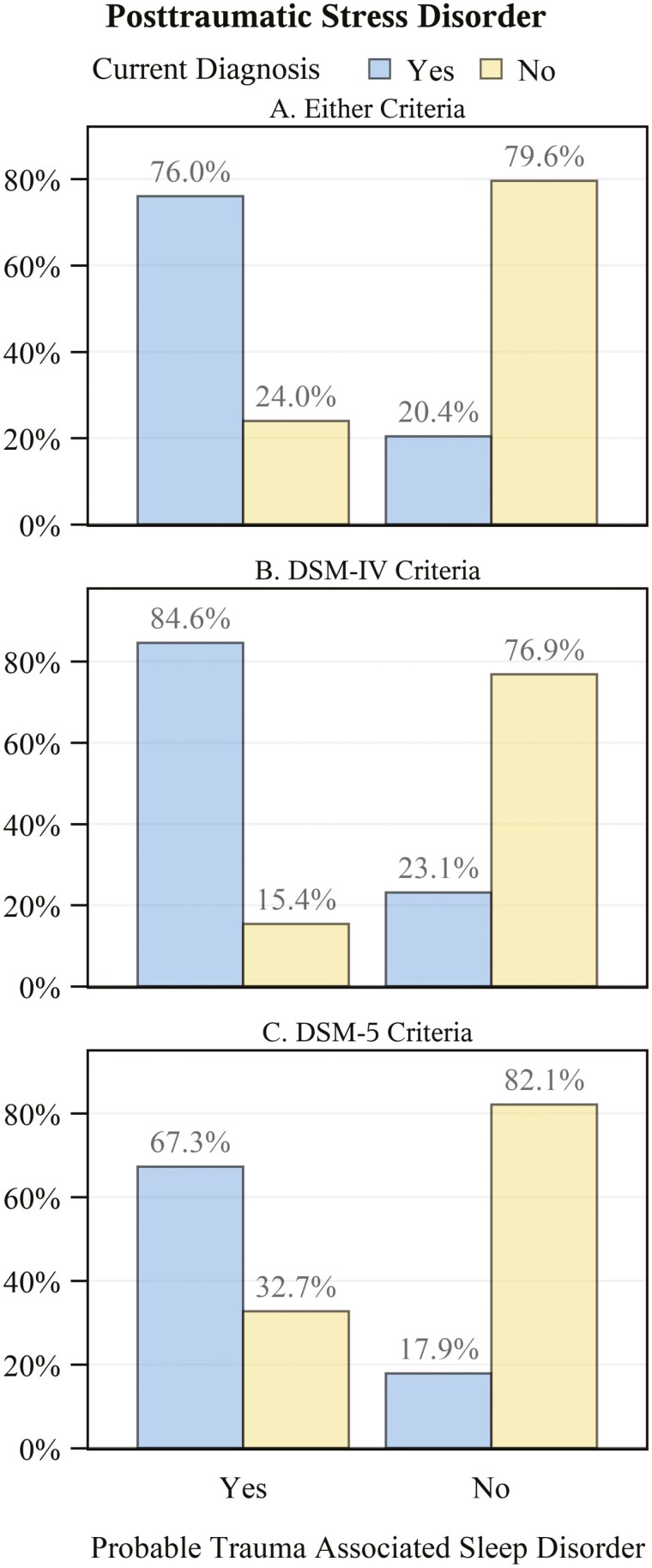
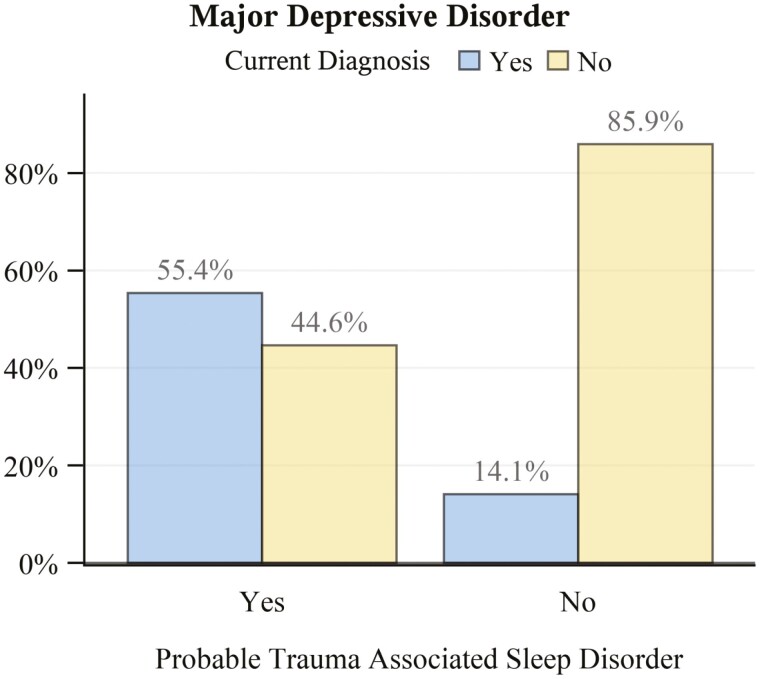
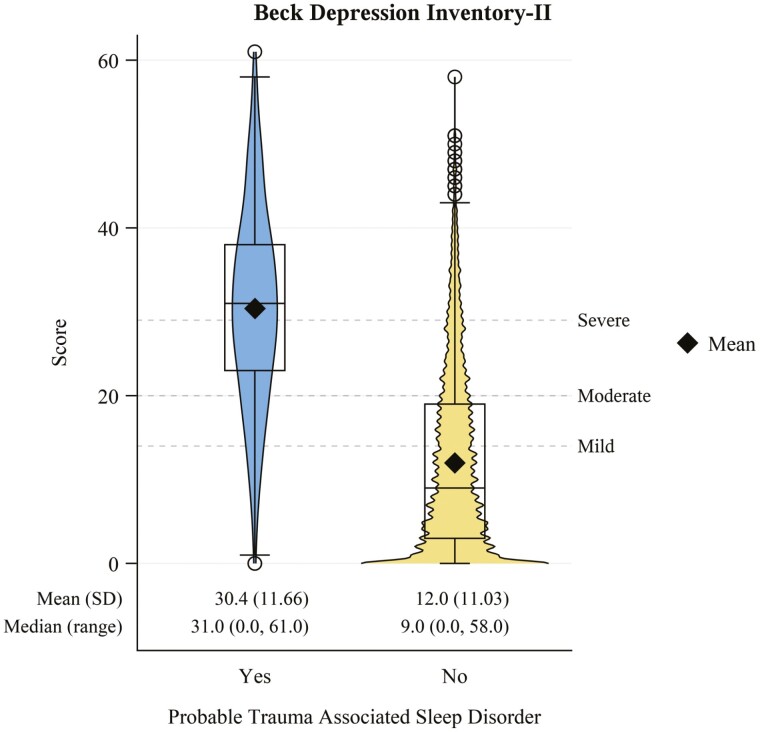
Results: Our final sample included 3618 veterans (22.7% female). TASD prevalence was 12.1% (95% CI: 11.1% to 13.2%) and sex-stratified prevalence was similar for female and male veterans. Veterans with TASD had a much higher comorbid prevalence of PTSD (PR: 3.72, 95% CI: 3.41 to 4.06) and MDD (PR: 3.93, 95% CI: 3.48 to 4.43). Combat was the highest reported most distressing traumatic experience among veterans with TASD (62.6%). When stratifying by sex, female veterans with TASD had a wider variety of traumatic experiences.
Conclusions: Our results support the need for improved screening and evaluation for TASD in veterans, which is currently not performed in routine clinical practice.
Keywords: combat; military; nightmares; parasomnias; sleep–wake disorders; trauma; trauma associated sleep disorder; veterans.
Published by Oxford University Press on behalf of Sleep Research Society 2023.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
