

Dysglycemias in patients admitted to ICUs with severe acute respiratory syndrome due to COVID-19 versus other causes - a cohort study
- PMID: 37193970
- PMCID: PMC10187505
- DOI: 10.1186/s12890-023-02439-y
Dysglycemias in patients admitted to ICUs with severe acute respiratory syndrome due to COVID-19 versus other causes - a cohort study
Abstract
Background: Dysglycemias have been associated with worse prognosis in critically ill patients with COVID-19, but data on the association of dysglycemia with COVID-19 in comparison with other forms of severe acute respiratory syndrome are lacking. This study aimed to compare the occurrence of different glycemic abnormalities in patients with severe acute respiratory syndrome and COVID-19 admitted to intensive care units versus glycemic abnormalities in patients with severe acute respiratory syndrome from other causes, to evaluate the adjusted attributable risk associated with COVID-19 and dysglycemia and to assess the influence of these dysglycemias on mortality.
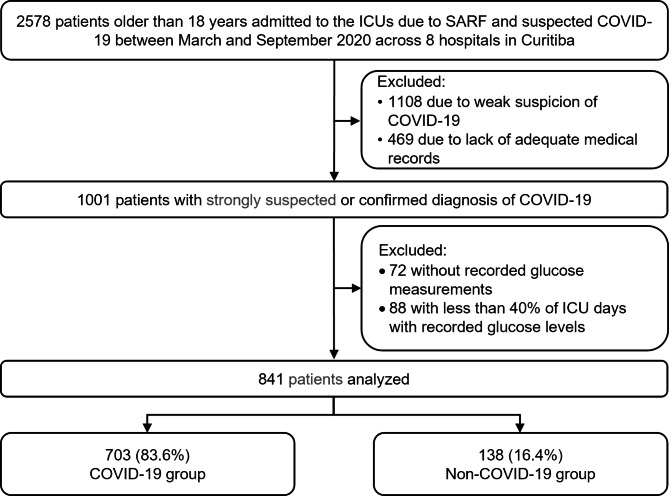
Methods: We conducted a retrospective cohort of consecutive patients with severe acute respiratory syndrome and suspected COVID-19 hospitalized in intensive care units between March 11 and September 13, 2020, across eight hospitals in Curitiba-Brazil. The primary outcome was the influence of COVID-19 on the variation of the following parameters of dysglycemia: highest glucose level at admission, mean and highest glucose levels during ICU stay, mean glucose variability, percentage of days with hyperglycemia, and hypoglycemia during ICU stay. The secondary outcome was the influence of COVID-19 and each of the six parameters of dysglycemia on hospital mortality within 30 days from ICU admission.
Results: The sample consisted of 841 patients, of whom 703 with and 138 without COVID-19. Comparing patients with and without COVID-19, those with COVID-19 had significantly higher glucose peaks at admission (165 mg/dL vs. 146 mg/dL; p = 0.002) and during ICU stay (242 mg/dL vs. 187md/dL; p < 0.001); higher mean daily glucose (149.7 mg/dL vs. 132.6 mg/dL; p < 0.001); higher percentage of days with hyperglycemia during ICU stay (42.9% vs. 11.1%; p < 0.001); and greater mean glucose variability (28.1 mg/dL vs. 25.0 mg/dL; p = 0.013). However, these associations were no longer statistically significant after adjustment for Acute Physiology and Chronic Health Evaluation II scores, Sequential Organ Failure Assessment scores, and C-reactive protein level, corticosteroid use and nosocomial infection. Dysglycemia and COVID-19 were each independent risk factors for mortality. The occurrence of hypoglycemia (< 70 mg/dL) during ICU stay was not associated with COVID-19.
Conclusion: Patients with severe acute respiratory syndrome due to COVID-19 had higher mortality and more frequent dysglycemia than patients with severe acute respiratory syndrome due to other causes. However, this association did not seem to be directly related to the SARS-CoV-2 infection.
Keywords: COVID-19; Critical illness; Glycemic control; Hyperglycemia; Intensive care units.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Aramendi I, Burghi G, Manzanares W. Dysglycemia in the critically ill patient: current evidence and future perspectives. Rev Bras Ter Intensiva [Internet]. 2017;29(3). Available from: http://www.gnresearch.org/doi/10.5935/0103-507X.20170054. - PMC - PubMed
-
- Krinsley JStephe. Glycemic control in the critically ill: What have we learned since NICE-SUGAR? Hosp Pract (1995) [Internet]. 2015 [cited 2022 Jul 4];43(3):191–7. Available from: https://pubmed.ncbi.nlm.nih.gov/26224425/. - PubMed
-
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc [Internet]. 2003 [cited 2022 Jul 4];78(12):1471–8. Available from: https://pubmed.ncbi.nlm.nih.gov/14661676/. - PubMed
-
- Yegneswaran B, Parket R, Gawel S, Pritchard-Bell A, Ho T, Clermont G. Association between average glucose levels and hospital mortality among critically ill patients. Crit Care [Internet]. 2013 Apr 19;17(S2):P458. Available from: https://ccforum.biomedcentral.com/articles/10.1186/cc12396.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
