

Live birth rates following individualized dosing algorithm of follitropin delta in a long GnRH agonist protocol
- PMID: 37194068
- PMCID: PMC10185461
- DOI: 10.1186/s12958-023-01090-w
Live birth rates following individualized dosing algorithm of follitropin delta in a long GnRH agonist protocol
Abstract
Purpose: To explore the efficacy and safety of individualized follitropin delta dosing, based on serum anti-Müllerian hormone (AMH) concentration and bodyweight, in a long gonadotropin-releasing hormone (GnRH) agonist protocol.
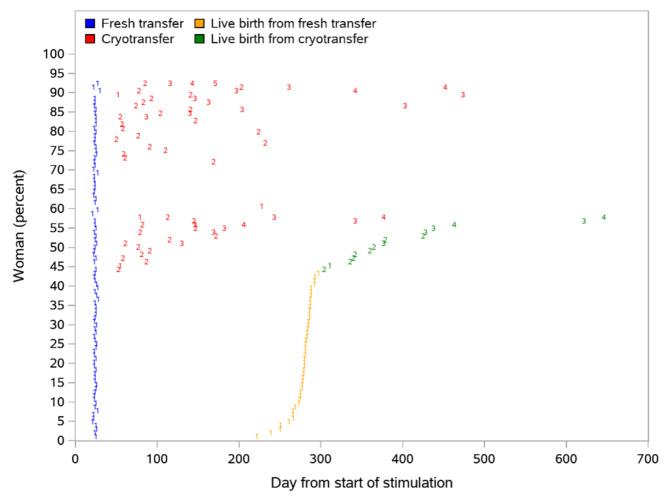
Methods: Clinical outcomes after one treatment cycle are reported in women with AMH: 5-35 pmol/L. Oocytes were inseminated by intracytoplasmic sperm injection, blastocyst transfer was on Day 5 and remaining blastocysts were cryopreserved. Data collection included live births and neonatal health follow-up for all fresh/frozen transfers performed within one year after treatment allocation.
Results: In total, 104 women started stimulation, of whom 101 had oocyte recovery and 92 had blastocyst transfer. The average daily dose of follitropin delta was 11.0 ± 1.6 µg and the duration of stimulation was 10.3 ± 1.6 days. The mean number of oocytes was 12.5 ± 6.4, the mean number of blastocysts was 5.1 ± 3.4, and 85% had at least one good-quality blastocyst. Following mostly single blastocyst transfer (95%), the ongoing pregnancy rate was 43%, the live-birth rate was 43%, and the cumulative live-birth rate was 58% per started stimulation. There were 6 cases of early OHSS (5.8%) graded as mild (n = 3) and moderate (n = 3) and 6 cases of late OHSS (5.8%) graded as moderate (n = 3) and severe (n = 3).
Conclusion: In this first evaluation of the individualized follitropin delta dosing in a long GnRH agonist protocol, the cumulative live-birth rate was high. A randomized trial comparing follitropin delta in a long GnRH agonist protocol versus in a GnRH antagonist protocol should provide further insight into the efficacy and safety of this treatment option.
Trial registration number: NCT03564509; June 21, 2018.
Keywords: Cumulative live birth rates; Follitropin delta; Individualized dosing; Long GnRH agonist.
© 2023. The Author(s).
Conflict of interest statement
M.F.S. has received grants and/or speaker fees from Ferring, Merck, Organon, MSD, Gedeon Richter, Theramex, IBSA. P.L. is an employee of Ferring Pharmaceuticals. M.F. has received consulting fees from Gedon Richter, speaker fees from Merck, MDS, Gedeon Richter and Ferring Pharmaceuticals, and has received support for attending meetings and/or travel from Ferring Pharmaceuticals, Merck, MSD, Gedeon Richter, IBSA, and Theramex. E.B. has received research funding from Roche Diagnostics and IBSA, a grant from Gedeon-Richter, speaker fees from Ferring Pharmaceticals, Merck, MSD, Gedeon-Richter, Roche Diagnostics and IBSA, and has participated in data safety monitoring/advisory board for Ferring Pharmaceuticals, Merck, MSD, Gedeon-Richter Roche Diagnostics, IBSA, and Abbott. J.A.G.V. has received grants and/or speaker fees from Ferring, Merck, Organon, MSD, Gedeon Richter, Theramex and IBSA. E.S.L. has no completing interests. B.M. was an employee of Ferring Pharmaceuticals at the time of the study.
Figures

References
-
- Youssef MA, Van der Veen F, Al-Inany HG, Mochtar MH, Griesinger G, Nagi Mohesen M, Aboulfoutouh I, van Wely M. Gonadotropin-releasing hormone agonist versus HCG for oocyte triggering in antagonist-assisted reproductive technology. Cochrane Database Syst Rev. 2014;CD008046. 10.1002/14651858.CD008046.pub4. - PMC - PubMed
-
- Arce JC, Andersen AN, Fernandez-Sanchez M, Visnova H, Bosch E, Garcia-Velasco JA, Barri P, de Sutter P, Klein BM, Fauser BC. Ovarian response to recombinant human follicle-stimulating hormone: a randomized, antimullerian hormone-stratified, dose-response trial in women undergoing in vitro fertilization/intracytoplasmic sperm injection. Fertil Steril. 2014;102:1633–1640e1635. doi: 10.1016/j.fertnstert.2014.08.013. - DOI - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
