

Therapy results in pediatric Hodgkin lymphoma - does less mean better? Experience from a single children's oncology center
- PMID: 37195291
- PMCID: PMC10345031
- DOI: 10.1007/s00277-023-05268-5
Therapy results in pediatric Hodgkin lymphoma - does less mean better? Experience from a single children's oncology center
Abstract
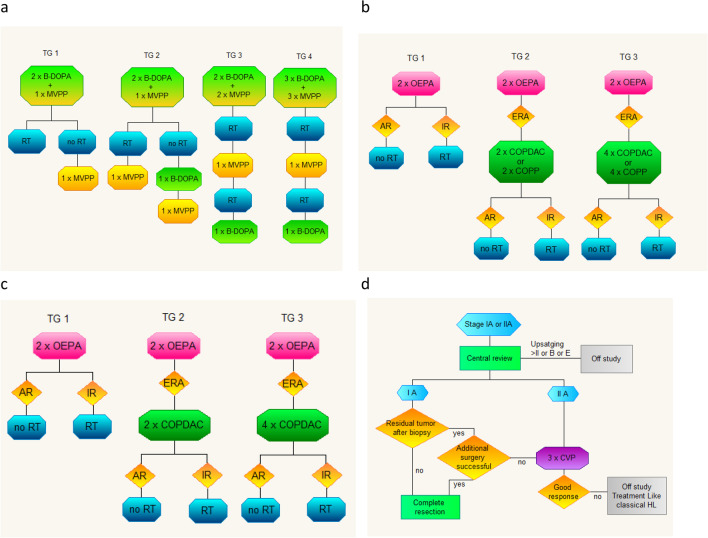
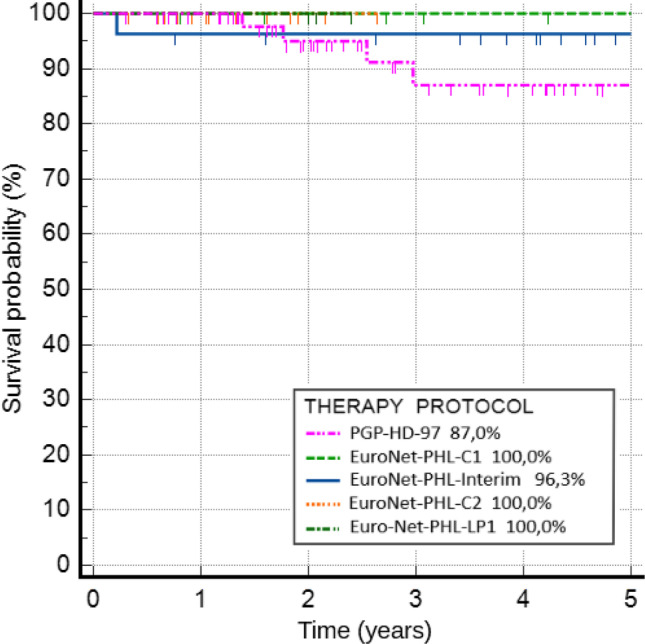
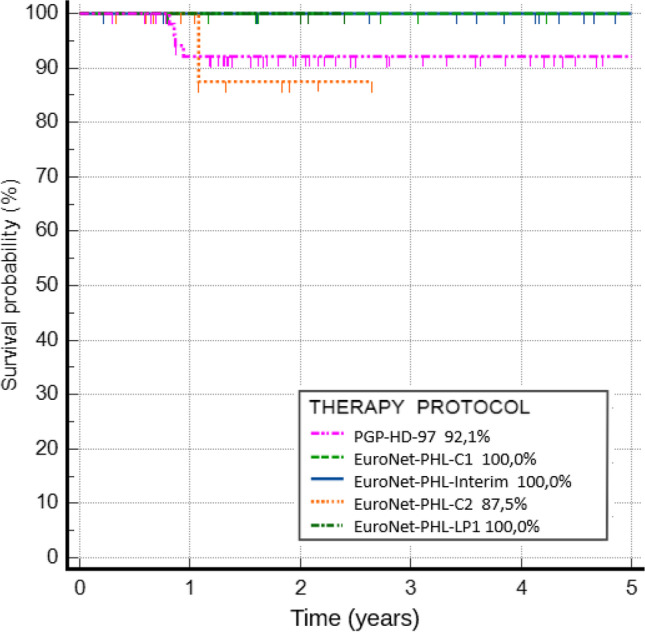
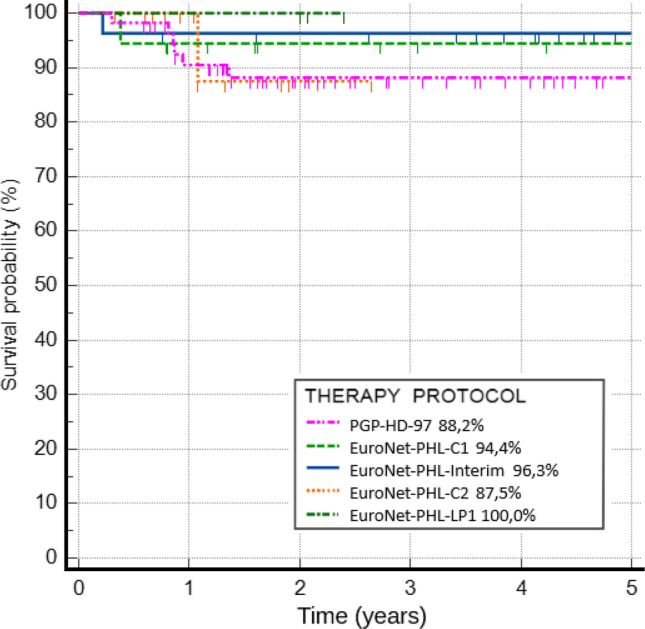
Therapy results in pediatric Hodgkin lymphoma reflect remarkable progress in pediatric oncology. In the last decade, relevant development of new therapeutic options for children with refractory or relapsed disease has been made. In this study, we retrospectively analyzed therapy results and risk factors in children treated in a single oncology center according to five therapeutic protocols. Data from 114 children treated by a single institution between 1997 and 2022 were analyzed. Classic Hodgkin lymphoma therapy results were divided into four therapeutic periods: 1997-2009, 2009-2014, 2014-2019, and 2019-2022. For nodular lymphocyte-predominant Hodgkin lymphoma, data from one therapeutic protocol was analyzed. For the entire group, the 5-year probability of overall survival was 93.5%. There were no statistically significant differences between therapeutic periods. The occurrence of B symptoms at diagnosis and incidence of relapse were risk factors for death (p = 0.018 and p < 0.001). Relapse occurred in 5 cases. The 5-year probability of relapse-free survival for the entire group was 95.2%, without significant differences between groups. Patients treated between 1997 and 2009 had over a sixfold higher risk for events, defined as primary progression, relapse, death, or incidence of secondary malignancies (OR = 6.25, p = 0.086). The 5-year probability of event-free survival for all patients was 91.3%. Five patients died, and the most common cause of death was relapse. Modern therapeutic protocols in pediatric Hodgkin lymphoma are marked by excellent outcomes. Patients with disease relapses have a notably high risk of death, and the development of new therapeutic options for this group remains one of the main goals of current trials.
Keywords: Children; Hodgkin lymphoma; Radiotherapy; Survival; Therapeutic era.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Balwierz W, Dzikowska K, Szurgot M, Klekawka T, Moryl-Bujakowska A. Postępy w leczeniu chłoniaka Hodgkina u dzieci i młodzieży. Acta Haematol Polonica. 2013;44(3):182–187. doi: 10.1016/j.achaem.2013.07.004. - DOI
-
- Harker-Murray P, Leblanc T, Mascarin M, Mauz-Körholz C, Michel G, Cooper S, et al. Response-adapted therapy with nivolumab and brentuximab vedotin (BV), followed by BV and bendamustine for suboptimal response, in children, adolescents, and young adults with standard-risk relapsed/refractory classical Hodgkin lymphoma. Blood. 2018;132:927. doi: 10.1182/blood-2018-99-111279. - DOI
-
- Kung FH, Schwartz CL, Ferree CR, London WB, Ternberg JL, Behm FG, et al. POG 8625: a randomized trial comparing chemotherapy with chemoradiotherapy for children and adolescents with Stages I, IIA, IIIA1 Hodgkin Disease: a report from the Children’s Oncology Group. J Pediatr Hematol Oncol. 2006;28:362–368. doi: 10.1097/00043426-200606000-00008. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
