

Comparative Genomic Landscape of Urothelial Carcinoma of the Bladder Among Patients of East and South Asian Genomic Ancestry
- PMID: 37196060
- PMCID: PMC10546831
- DOI: 10.1093/oncolo/oyad120
Comparative Genomic Landscape of Urothelial Carcinoma of the Bladder Among Patients of East and South Asian Genomic Ancestry
Abstract
Background: Despite the low rate of urothelial carcinoma of the bladder (UCB) in patients of South Asian (SAS) and East Asian (EAS) descent, they make up a significant portion of the cases worldwide. Nevertheless, these patients are largely under-represented in clinical trials. We queried whether UCB arising in patients with SAS and EAS ancestry would have unique genomic features compared to the global cohort.
Methods: Formalin-fixed, paraffin-embedded tissue was obtained for 8728 patients with advanced UCB. DNA was extracted and comprehensive genomic profiling was performed. Ancestry was classified using a proprietary calculation algorithm. Genomic alterations (GAs) were determined using a 324-gene hybrid-capture-based method which also calculates tumor mutational burden (TMB) and determines microsatellite status (MSI).
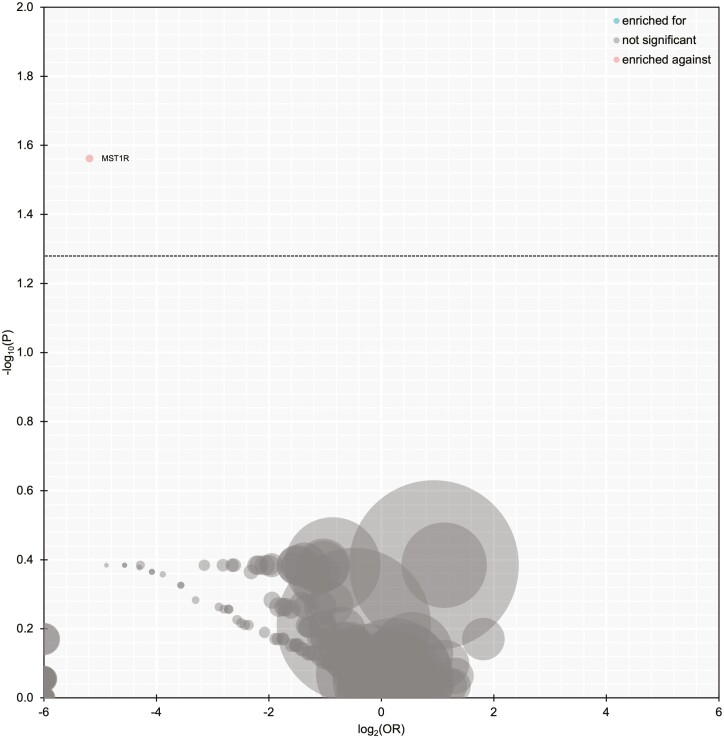
Results: Of the cohort, 7447 (85.3%) were EUR, 541 (6.2%) were AFR, 461 (5.3%) were of AMR, 74 (0.85%) were SAS, and 205 (2.3%) were EAS. When compared with EUR, TERT GAs were less frequent in SAS (58.1% vs. 73.6%; P = .06). When compared with non-SAS, SAS had less frequent GAs in FGFR3 (9.5% vs. 18.5%, P = .25). TERT promoter mutations were significantly less frequent in EAS compared to non-EAS (54.1% vs. 72.9%; P < .001). When compared with the non-EAS, PIK3CA alterations were significantly less common in EAS (12.7% vs. 22.1%, P = .005). The mean TMB was significantly lower in EAS vs. non-EAS (8.53 vs. 10.02; P = .05).
Conclusions: The results from this comprehensive genomic analysis of UCB provide important insight into the possible differences in the genomic landscape in a population level. These hypothesis-generating findings require external validation and should support the inclusion of more diverse patient populations in clinical trials.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
Roger Li: Predicine, Veracyte, CG Oncology, Valar Labs (research support), CG Oncology (clinical trial protocol committee), BMS, Merck, Fergene, Arquer Diagnostics, Urogen Pharma, Lucence (scientific advisor/consultant). Petros Grivas: Aadi Bioscience, AstraZeneca, Astellas Pharma, Boston Gene, Bristol Myers Squibb, CG Oncology Inc., Dyania Health, EMD Serono, Exelixis, Fresenius Kabi, Genentech/Roche, Gilead Sciences, Guardant Health, Infinity Pharmaceuticals, Janssen, Lucence Health, MSD, Mirati Therapeutics, Pfizer, PureTech, QED Therapeutics, Regeneron Pharmaceuticals, Seattle Genetics, Silverback Therapeutics, 4D Pharma PLC, UroGen (consulting), Bavarian Nordic, Bristol Myers Squibb, Clovis Oncology, Debiopharm, EMD Serono, G1 Therapeutics, Gilead Sciences, GlaxoSmithKline, MSD, Mirati Therapeutics, Pfizer, QED Therapeutics (institutional research funding). Andrea Necchi: Merck, AstraZeneca, Janssen, Incyte, Roche, Rainier Therapeutics, Clovis Oncology, Bayer, Astellas/Seattle Genetics, Ferring, Immunomedics (consulting/advisory relationships), Merck, Ipsen, AstraZeneca (research funding). Dean Pavlick, Richard S.P. Huang, Douglas Lin, Natalie Danziger, Jeffrey S. Ross: Foundation Medicine Inc., a wholly owned subsidiary of Roche (employment) and Roche (ownership interest). Joseph M. Jacob: Janssen and Urogen (consulting). Taylor Peak, Philippe E. Spiess, and Gennady Bratslavsky indicated no financial relationships.
Figures





References
-
- Hoffman-Censits J, Kanesvaran R, Bangs R, Fashoyin-Aje L, Weinstock C.. Breaking barriers: addressing issues of inequality in trial enrollment and clinical outcomes for patients with kidney and bladder cancer. Am Soc Clin Oncol Educ Book. 2021;41:e174-ee81. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
