

Effect of Histopathological Explanations for Dermoscopic Criteria on Learning Curves in Skin Cancer Training: a Randomized Controlled Trial
- PMID: 37196312
- PMCID: PMC10188176
- DOI: 10.5826/dpc.1302a105
Effect of Histopathological Explanations for Dermoscopic Criteria on Learning Curves in Skin Cancer Training: a Randomized Controlled Trial
Abstract
Introduction: Case-based training improves novices pattern recognition and diagnostic accuracy in skin cancer diagnostics. However, it is unclear how pattern recognition is best taught in conjunction with the knowledge needed to justify a diagnosis.
Objectives: The aim of this study was to examine whether an explanation of the underlying histopathological reason for dermoscopic criteria improves skill acquisition and retention during case-based training in skin cancer diagnostics.
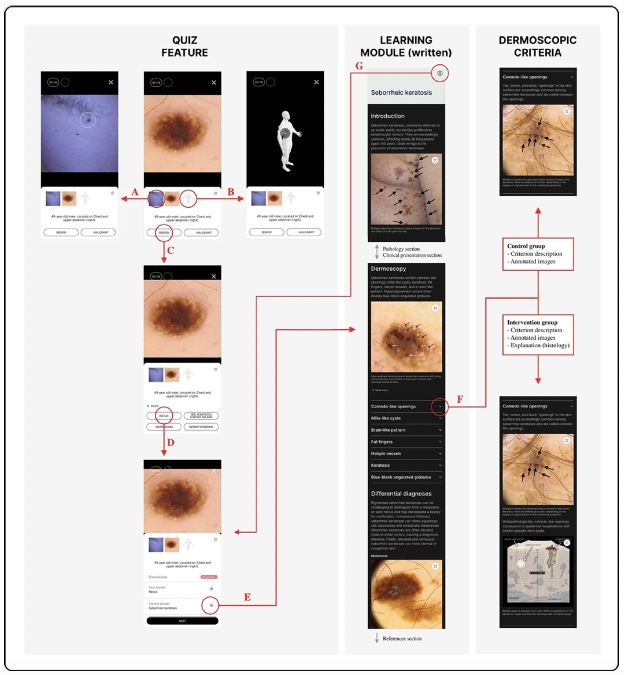
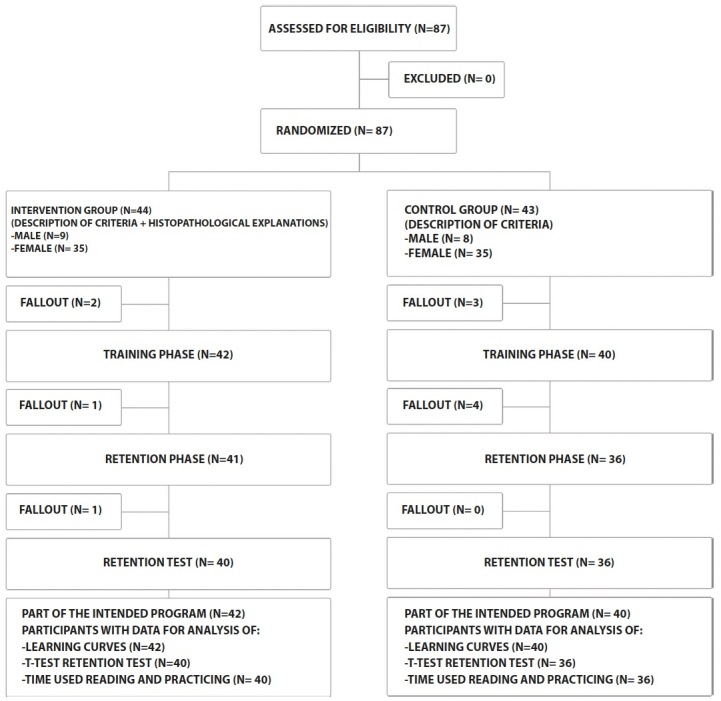
Methods: In this double-blinded randomized controlled trial, medical students underwent eight days of case-based training in skin cancer diagnostics, which included access to written diagnosis modules. The modules dermoscopic subsections differed between the study groups. All participants received a general description of the criteria, but the intervention group additionally received a histopathological explanation.
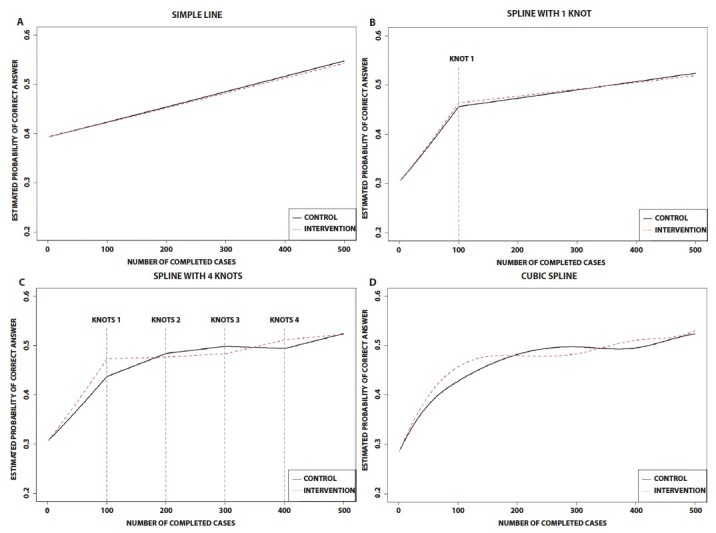
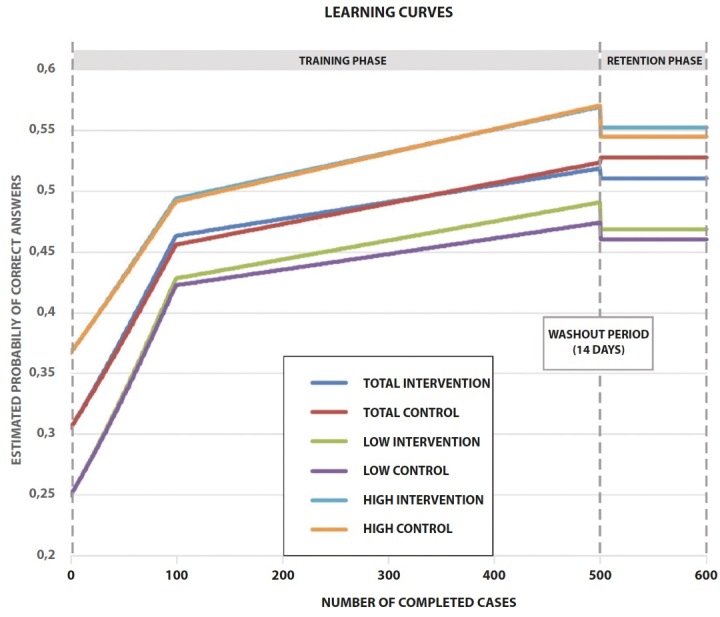
Results: Most participants (78%) passed a reliable test in skin cancer diagnostics, following a mean training time of 217 minutes. Access to histopathological explanations did not affect participants' learning curves or skill retention.
Conclusions: The histopathological explanation did not affect the students, but the overall educational approach was efficient and scalable.
Conflict of interest statement
Figures

Similar articles
-
Improving Skin Cancer Diagnostics Through a Mobile App With a Large Interactive Image Repository: Randomized Controlled Trial.JMIR Dermatol. 2023 Aug 9;6:e48357. doi: 10.2196/48357. JMIR Dermatol. 2023. PMID: 37624707 Free PMC article.
-
Effect of Continuous Motion Parameter Feedback on Laparoscopic Simulation Training: A Prospective Randomized Controlled Trial on Skill Acquisition and Retention.J Surg Educ. 2018 Mar-Apr;75(2):516-526. doi: 10.1016/j.jsurg.2017.08.015. Epub 2017 Aug 31. J Surg Educ. 2018. PMID: 28864265 Clinical Trial.
-
The effect of direct referral for fast CT scan in early lung cancer detection in general practice. A clinical, cluster-randomised trial.Dan Med J. 2015 Mar;62(3):B5027. Dan Med J. 2015. PMID: 25748876 Clinical Trial.
-
Take-Home Training in Laparoscopy.Dan Med J. 2017 Apr;64(4):B5335. Dan Med J. 2017. PMID: 28385174 Review.
-
Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy.Cochrane Database Syst Rev. 2018 Aug 17;8(8):CD008237. doi: 10.1002/14651858.CD008237.pub3. Cochrane Database Syst Rev. 2018. PMID: 30117156 Free PMC article.
Cited by
-
Improving Skin Cancer Diagnostics Through a Mobile App With a Large Interactive Image Repository: Randomized Controlled Trial.JMIR Dermatol. 2023 Aug 9;6:e48357. doi: 10.2196/48357. JMIR Dermatol. 2023. PMID: 37624707 Free PMC article.
-
The effects of procedural and conceptual knowledge on visual learning.Adv Health Sci Educ Theory Pract. 2024 Sep;29(4):1243-1263. doi: 10.1007/s10459-023-10304-0. Epub 2023 Dec 7. Adv Health Sci Educ Theory Pract. 2024. PMID: 38060072 Free PMC article.
References
-
- Tschandl P, Codella N, Akay BN, et al. Comparison of the accuracy of human readers versus machine-learning algorithms for pigmented skin lesion classification: an open, web-based, international, diagnostic study. Lancet Oncol. 2019;20(7):938–947. doi: 10.1016/S1470-2045(19)30333-X. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources