

Relapsing immunoglobulin G4-related sclerosing cholangitis during maintenance treatment with low-dose steroids: a case report
- PMID: 37197250
- PMCID: PMC10184037
- DOI: 10.21037/tgh-21-111
Relapsing immunoglobulin G4-related sclerosing cholangitis during maintenance treatment with low-dose steroids: a case report
Abstract
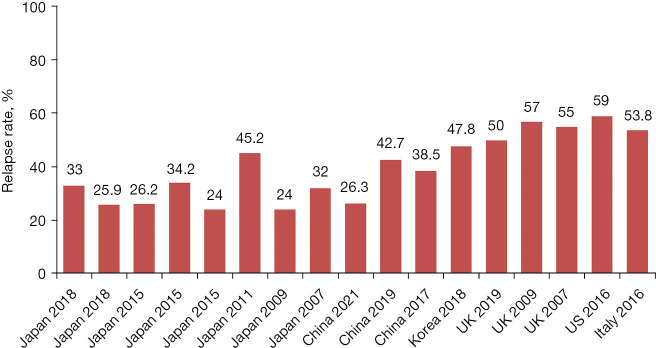
Background: Immunoglobulin G4-related sclerosing cholangitis (IgG4-SC) often has a good response to initial steroid therapy, but a high relapse rate during follow-up. Knowledge about the predictors and treatment strategy of relapsing IgG4-SC is of great significance.
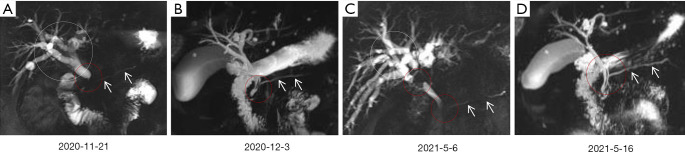
Case description: In this paper, we reported that a 57-year-old male was diagnosed with IgG4-SC accompanied by type 1 autoimmune pancreatitis (AIP) at the first onset of his diseases and had a good response to steroid therapy. However, during low-dose steroids maintenance therapy, IgG4-SC relapsed with clinical presentations related to severe bile duct stricture, but improved rapidly after re-administration of full-dose steroids, accompanied by resolution of jaundice, improvement of intrahepatic and extrahepatic bile duct stricture, and gradual recovery of liver function. At the last follow-up in December 2021, he was still stable with methylprednisolone tablets at 4 mg/day.
Conclusions: IgG4-SC is likely to relapse in patients who have high serum IgG4 level at initial onset and receive low-dose steroids maintenance treatment. The predictors of disease relapse also include steroids interruption, more severe bile duct stricture, long duration from diagnosis to treatment, history of allergy, and high serum tumor necrosis factor-alpha (TNF-alpha) and soluble interleukin-2 receptor (sIL-2R) levels. Re-administration or up-dose of steroids, immunosuppressors, and rituximab are effective for treating relapsing disease.
Keywords: Immunoglobulin G4-related sclerosing cholangitis (IgG4-SC); case report; immunoglobulin G4-related disease (IgG4-RD); relapse; steroid.
2023 Translational Gastroenterology and Hepatology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tgh.amegroups.com/article/view/10.21037/tgh-21-111/coif). The authors have no conflicts of interest to declare.
Figures


Similar articles
-
Comparison of the long-term outcomes between proximal and distal IgG4-related sclerosing cholangitis: A multicenter cohort study.J Gastroenterol Hepatol. 2023 Apr;38(4):648-655. doi: 10.1111/jgh.16136. Epub 2023 Feb 9. J Gastroenterol Hepatol. 2023. PMID: 36710432 Review.
-
[Clinical observation of isolated immunoglobulin G4-related sclerosing cholangitis and immunoglobulin G4 sclerosing cholangitis combined autoimmune pancreatitis].Zhonghua Gan Zang Bing Za Zhi. 2018 Jun 20;26(6):415-419. doi: 10.3760/cma.j.issn.1007-3418.2018.06.005. Zhonghua Gan Zang Bing Za Zhi. 2018. PMID: 30317753 Chinese.
-
Clinical features of isolated proximal-type immunoglobulin G4-related sclerosing cholangitis.Dig Endosc. 2019 Jul;31(4):422-430. doi: 10.1111/den.13320. Epub 2019 Feb 11. Dig Endosc. 2019. PMID: 30570170
-
Immunosuppressant treatment for IgG4-related sclerosing cholangitis: A case report.World J Clin Cases. 2021 Jan 6;9(1):267-273. doi: 10.12998/wjcc.v9.i1.267. World J Clin Cases. 2021. PMID: 33511195 Free PMC article.
-
Endoscopic retrograde cholangiopancreatography and intraductal ultrasonography in the diagnosis of autoimmune pancreatitis and IgG4-related sclerosing cholangitis.J Med Ultrason (2001). 2021 Oct;48(4):573-580. doi: 10.1007/s10396-021-01114-1. Epub 2021 Jul 31. J Med Ultrason (2001). 2021. PMID: 34331625 Review.
Cited by
-
Successful Use of a Novel High-Dose Mycophenolate Mofetil and Rituximab Regimen for Progressive IgG4 Sclerosing Cholangitis With Multisystemic Involvement.ACG Case Rep J. 2025 Apr 16;12(4):e01672. doi: 10.14309/crj.0000000000001672. eCollection 2025 Apr. ACG Case Rep J. 2025. PMID: 40242299 Free PMC article.
-
Case report: Isolated immunoglobulin G4-related sclerosing cholangitis misdiagnosed as hilar cholangiocarcinoma.Front Oncol. 2024 May 23;14:1385214. doi: 10.3389/fonc.2024.1385214. eCollection 2024. Front Oncol. 2024. PMID: 38846973 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous