

Influence of hepatic dysfunction in patients who underwent tricuspid valve surgery
- PMID: 37197498
- PMCID: PMC10183499
- DOI: 10.21037/jtd-22-1741
Influence of hepatic dysfunction in patients who underwent tricuspid valve surgery
Erratum in
-
Erratum: Influence of hepatic dysfunction in patients who underwent tricuspid valve surgery.J Thorac Dis. 2024 Dec 31;16(12):8836. doi: 10.21037/jtd-2024-05. Epub 2024 Dec 28. J Thorac Dis. 2024. PMID: 39831251 Free PMC article.
Abstract
Background: Hepatic dysfunction (HD) is frequently associated with chronic tricuspid regurgitation (TR), and is a risk factor for TR surgery. Late referral of patients with TR is associated with the progression of TR and HD, as well as an increase in surgical morbidity and mortality. Many patients with severe TR suffer from HD; however, their clinical impact is not well documented.
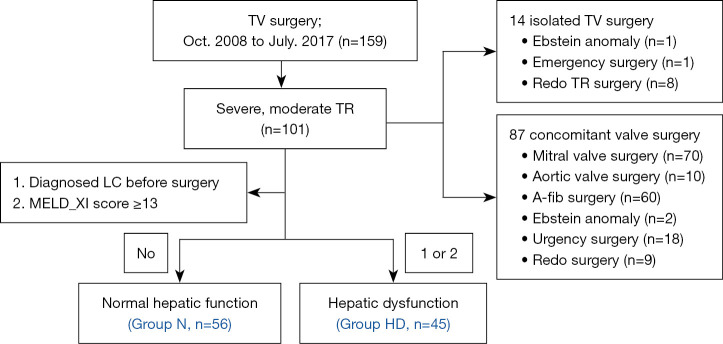
Methods: This retrospective review was conducted between October 2008 and July 2017. In total, 159 consecutive patients underwent surgery for TR; 101 with moderate to severe TR were included. We divided patients into N (normal liver function; n=56) and HD (HD; n=45) groups. HD was defined as clinically or radiologically diagnosed liver cirrhosis, or a preoperative Model for End-Stage Liver Disease (MELD)-XI score ≥13. Perioperative data were compared between groups, and changes in the MELD score following TR surgery were estimated in the HD group. Long-term survival rates were analyzed, and analyses were performed to obtain the assessment tool and cutoff value to determine the degree of HD affecting late mortality.
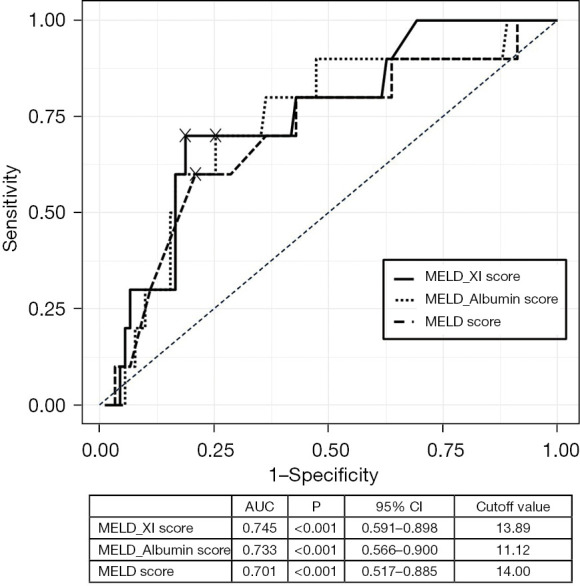
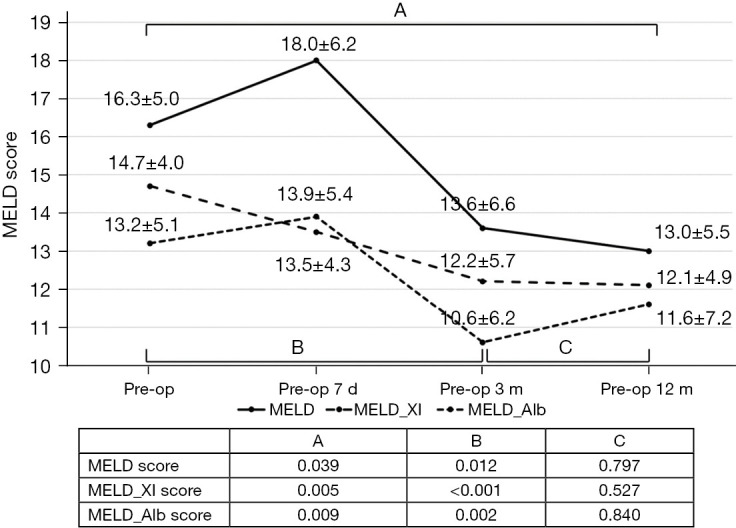
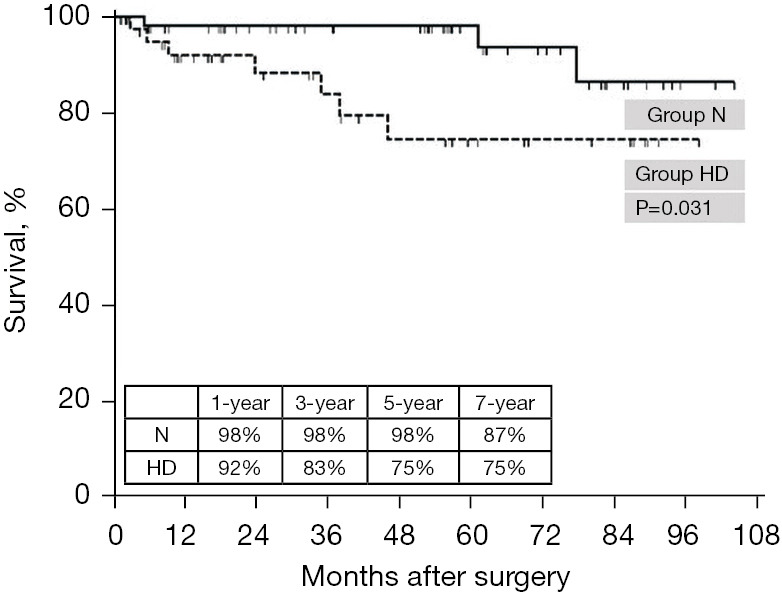
Results: The preoperative demographics of both groups were similar, excluding the presence of HD. The EuroSCORE II, MELD score, and prothrombin time international normalization ratio were significantly higher in the HD group, and although early mortality was comparable between groups [N group: 0%, HD group: 2.2% (n=1); P=0.446], intensive care unit and hospital stays were significantly longer in the HD group. The MELD score in the HD group temporarily increased immediately after surgery, and then decreased. The long-term survival rates were significantly lower in the HD group. The most suitable tool for predicting late mortality was the MELD-XI score, with a cutoff value of 13 points.
Conclusions: Surgery for patients with severe TR can be performed with relatively low morbidity and operative mortality, regardless of associated HD. MELD scores significantly improved after TR surgery in patients with HD. Even with favorable early outcomes, compromised long-term survival with HD suggests the need to develop an assessment tool that can evaluate the appropriate timing for TR surgery.
Keywords: Hepatic dysfunction; MELD score; tricuspid regurgitation; tricuspid valve surgery.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1741/coif). The authors have no conflicts of interest to declare.
Figures

Comment in
-
Detailed association between hepatic dysfunction and tricuspid valve surgery.J Thorac Dis. 2023 Sep 28;15(9):5258-5259. doi: 10.21037/jtd-23-1020. Epub 2023 Aug 30. J Thorac Dis. 2023. PMID: 37868847 Free PMC article. No abstract available.
Similar articles
-
Prognostic value of modified model for end-stage liver disease scores in patients with significant tricuspid regurgitation.Eur Heart J Qual Care Clin Outcomes. 2023 Apr 26;9(3):227-239. doi: 10.1093/ehjqcco/qcac027. Eur Heart J Qual Care Clin Outcomes. 2023. PMID: 35612991
-
Risk stratification for isolated tricuspid valve surgery assisted using the Model for End-Stage Liver Disease score.J Thorac Cardiovasc Surg. 2023 Nov;166(5):1433-1441.e1. doi: 10.1016/j.jtcvs.2021.11.102. Epub 2022 Mar 12. J Thorac Cardiovasc Surg. 2023. PMID: 35431033
-
Prognostic Value of Hepatorenal Function By Modified Model for End-stage Liver Disease (MELD) Score in Patients Undergoing Tricuspid Annuloplasty.J Am Heart Assoc. 2018 Jul 13;7(14):e009020. doi: 10.1161/JAHA.118.009020. J Am Heart Assoc. 2018. PMID: 30006492 Free PMC article.
-
Which patient undergoing mitral valve surgery should also have the tricuspid repair?Interact Cardiovasc Thorac Surg. 2009 Dec;9(6):1009-20. doi: 10.1510/icvts.2009.217570. Epub 2009 Sep 24. Interact Cardiovasc Thorac Surg. 2009. PMID: 19778956 Review.
-
Isolated functional tricuspid regurgitation: When should we go to surgical treatment?J Cardiol. 2020 Apr;75(4):339-343. doi: 10.1016/j.jjcc.2019.11.001. Epub 2019 Nov 29. J Cardiol. 2020. PMID: 31787551 Review.
Cited by
-
If a job's worth doing, it's worth doing well at optimal timing.J Thorac Dis. 2023 Sep 28;15(9):5260-5261. doi: 10.21037/jtd-2023-10. Epub 2023 Sep 4. J Thorac Dis. 2023. PMID: 37868888 Free PMC article. No abstract available.
-
N-acetyl Cysteine to Mitigate Liver Damage in Patients with Deranged Liver Function Undergoing Surgery on Cardiopulmonary Bypass.Ann Card Anaesth. 2024 Oct 1;27(4):299-300. doi: 10.4103/aca.aca_156_24. Epub 2024 Oct 4. Ann Card Anaesth. 2024. PMID: 39365126 Free PMC article. No abstract available.
-
Erratum: Influence of hepatic dysfunction in patients who underwent tricuspid valve surgery.J Thorac Dis. 2024 Dec 31;16(12):8836. doi: 10.21037/jtd-2024-05. Epub 2024 Dec 28. J Thorac Dis. 2024. PMID: 39831251 Free PMC article.
-
Detailed association between hepatic dysfunction and tricuspid valve surgery.J Thorac Dis. 2023 Sep 28;15(9):5258-5259. doi: 10.21037/jtd-23-1020. Epub 2023 Aug 30. J Thorac Dis. 2023. PMID: 37868847 Free PMC article. No abstract available.
-
Novel risk prediction model for major adverse cardiovascular events in minimally invasive mitral valve surgery: a retrospective study.Cardiovasc Diagn Ther. 2025 Jun 30;15(3):550-562. doi: 10.21037/cdt-2025-25. Epub 2025 Jun 26. Cardiovasc Diagn Ther. 2025. PMID: 40656786 Free PMC article.
References
-
- Iino K, Takemura H. Cardiac surgery for patients with liver cirrhosis. Kyobu Geka 2017;70:596-600. - PubMed
LinkOut - more resources
Full Text Sources