

Retained Metabolic Flexibility of the Failing Human Heart
- PMID: 37199155
- PMCID: PMC10417210
- DOI: 10.1161/CIRCULATIONAHA.122.062166
Retained Metabolic Flexibility of the Failing Human Heart
Abstract
Background: The failing heart is traditionally described as metabolically inflexible and oxygen starved, causing energetic deficit and contractile dysfunction. Current metabolic modulator therapies aim to increase glucose oxidation to increase oxygen efficiency of adenosine triphosphate production, with mixed results.
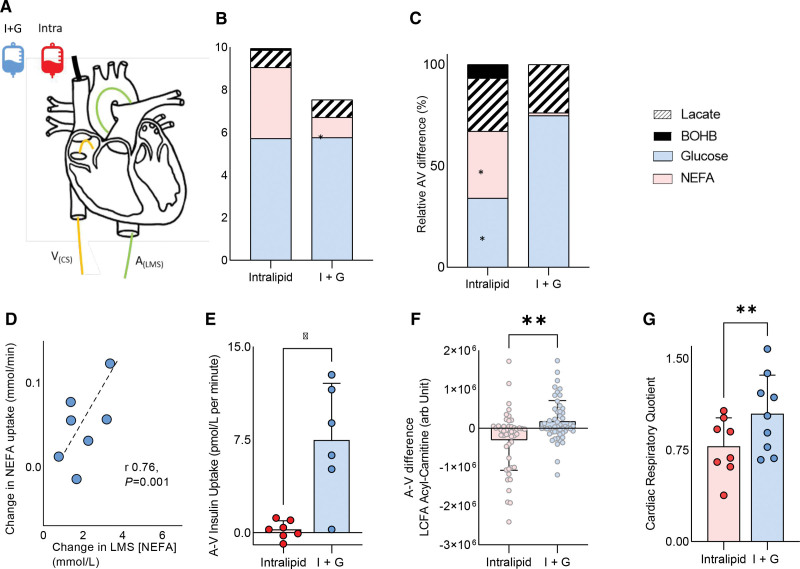
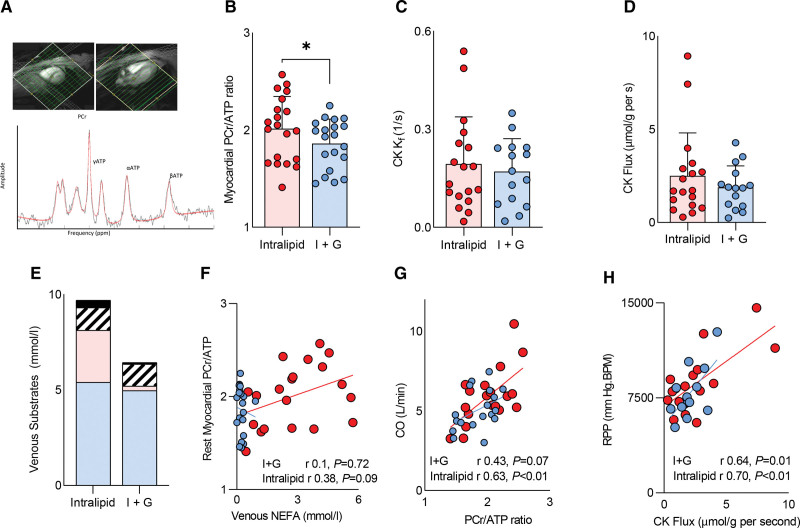
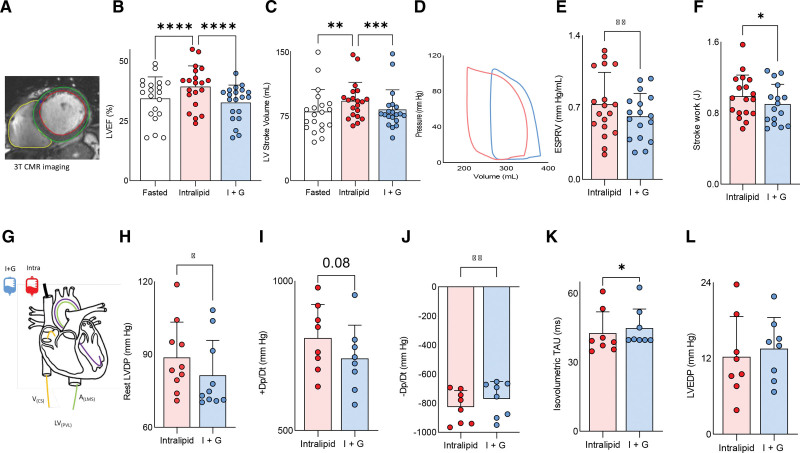
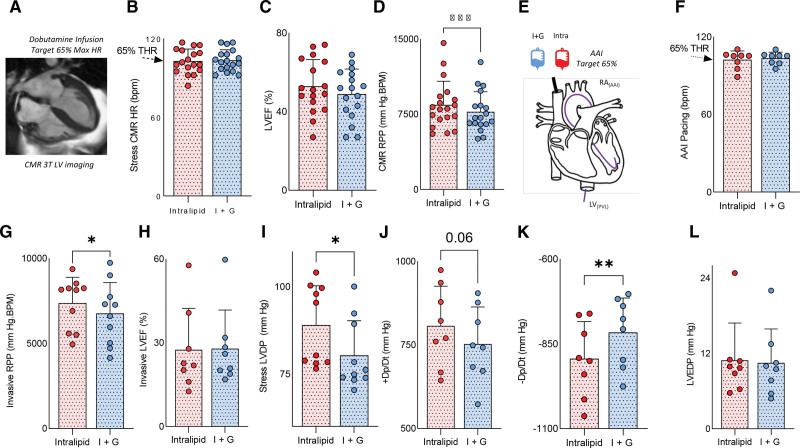
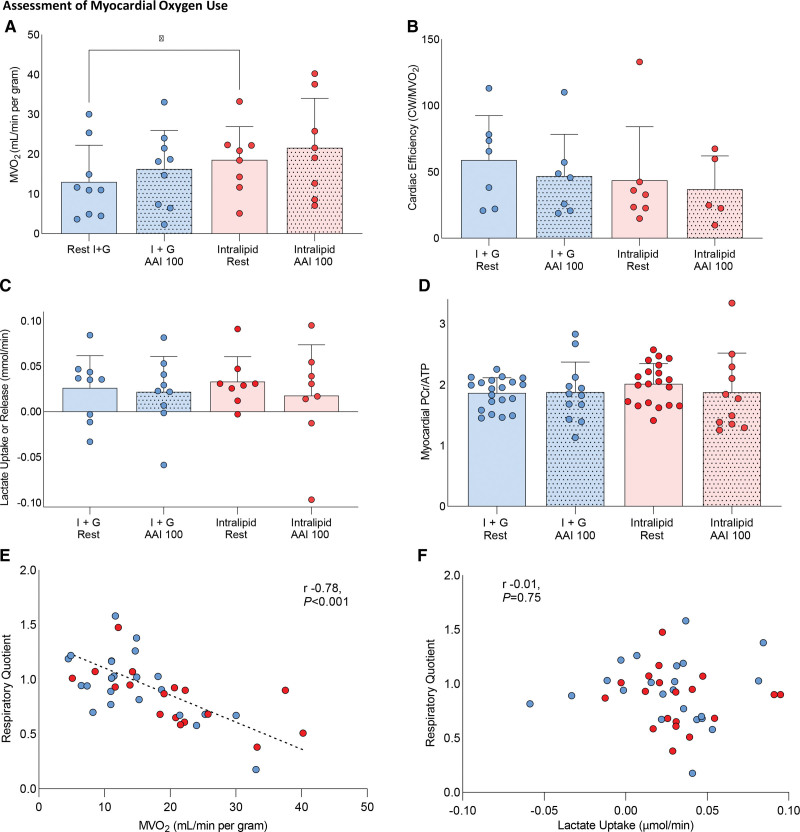
Methods: To investigate metabolic flexibility and oxygen delivery in the failing heart, 20 patients with nonischemic heart failure with reduced ejection fraction (left ventricular ejection fraction 34.9±9.1) underwent separate infusions of insulin+glucose infusion (I+G) or Intralipid infusion. We used cardiovascular magnetic resonance to assess cardiac function and measured energetics using phosphorus-31 magnetic resonance spectroscopy. To investigate the effects of these infusions on cardiac substrate use, function, and myocardial oxygen uptake (MVo2), invasive arteriovenous sampling and pressure-volume loops were performed (n=9).
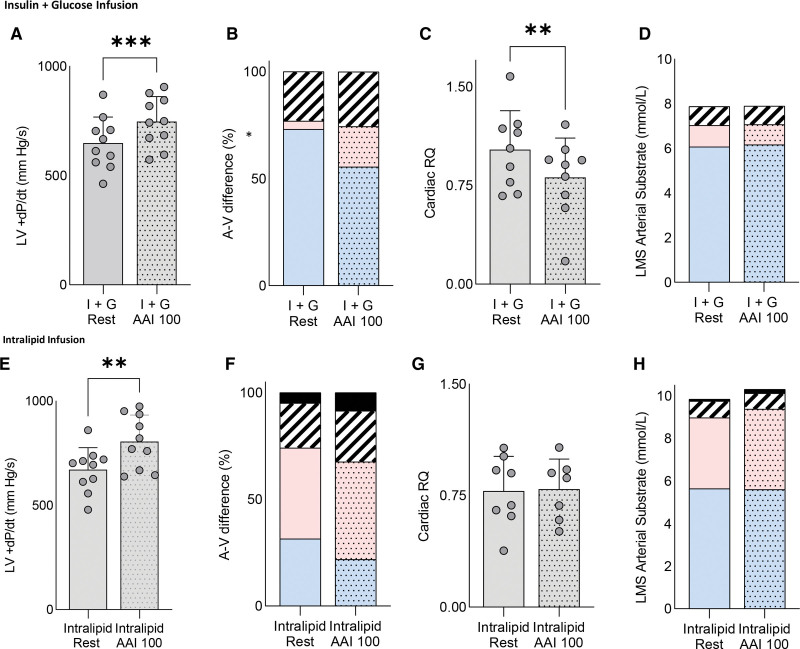
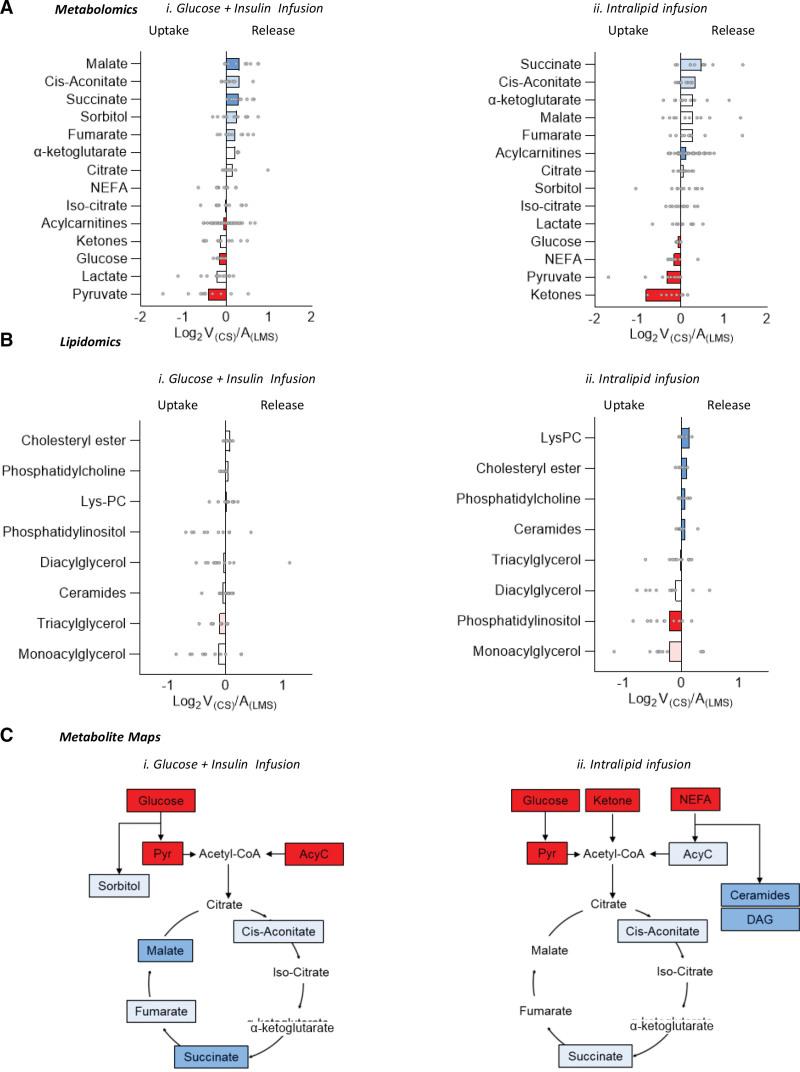
Results: At rest, we found that the heart had considerable metabolic flexibility. During I+G, cardiac glucose uptake and oxidation were predominant (70±14% total energy substrate for adenosine triphosphate production versus 17±16% for Intralipid; P=0.002); however, no change in cardiac function was seen relative to basal conditions. In contrast, during Intralipid infusion, cardiac long-chain fatty acid (LCFA) delivery, uptake, LCFA acylcarnitine production, and fatty acid oxidation were all increased (LCFA 73±17% of total substrate versus 19±26% total during I+G; P=0.009). Myocardial energetics were better with Intralipid compared with I+G (phosphocreatine/adenosine triphosphate 1.86±0.25 versus 2.01±0.33; P=0.02), and systolic and diastolic function were improved (LVEF 34.9±9.1 baseline, 33.7±8.2 I+G, 39.9±9.3 Intralipid; P<0.001). During increased cardiac workload, LCFA uptake and oxidation were again increased during both infusions. There was no evidence of systolic dysfunction or lactate efflux at 65% maximal heart rate, suggesting that a metabolic switch to fat did not cause clinically meaningful ischemic metabolism.
Conclusions: Our findings show that even in nonischemic heart failure with reduced ejection fraction with severely impaired systolic function, significant cardiac metabolic flexibility is retained, including the ability to alter substrate use to match both arterial supply and changes in workload. Increasing LCFA uptake and oxidation is associated with improved myocardial energetics and contractility. Together, these findings challenge aspects of the rationale underlying existing metabolic therapies for heart failure and suggest that strategies promoting fatty acid oxidation may form the basis for future therapies.
Keywords: adenosine triphosphate; heart failure; magnetic resonance spectroscopy; metabolism.
Conflict of interest statement
Figures
References
-
- Peterzan MA, Lygate CA, Neubauer S, Rider OJ. Metabolic remodeling in hypertrophied and failing myocardium: a review. Am J Physiol Heart Circ Physiol. 2017;313:H597–H616. doi: 10.1152/ajpheart.00731.2016 - PubMed
-
- Heather LC, Cole MA, Lygate CA, Evans RD, Stuckey DJ, Murray AJ, Neubauer S, Clarke K. Fatty acid transporter levels and palmitate oxidation rate correlate with ejection fraction in the infarcted rat heart. Cardiovasc Res. 2006;72:430–437. doi: 10.1016/j.cardiores.2006.08.020 - PubMed
-
- Osorio JC, Stanley WC, Linke A, Castellari M, Diep QN, Panchal AR, Hintze TH, Lopaschuk GD, Recchia FA. Impaired myocardial fatty acid oxidation and reduced protein expression of retinoid X receptor-alpha in pacing-induced heart failure. Circulation. 2002;106:606–612. doi: 10.1161/01.cir.0000023531.22727.c1 - PubMed
-
- Davila-Roman VG, Vedala G, Herrero P, de las Fuentes L, Rogers JG, Kelly DP, Gropler RJ. Altered myocardial fatty acid and glucose metabolism in idiopathic dilated cardiomyopathy. J Am Coll Cardiol. 2002;40:271–277. doi: 10.1016/s0735-1097(02)01967-8 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
