

Busulfan Interlaboratory Proficiency Testing Program Revealed Worldwide Errors in Drug Quantitation and Dose Recommendations
- PMID: 37199431
- PMCID: PMC10635345
- DOI: 10.1097/FTD.0000000000001107
Busulfan Interlaboratory Proficiency Testing Program Revealed Worldwide Errors in Drug Quantitation and Dose Recommendations
Abstract
Background: The clinical outcomes of busulfan-based conditioning regimens for hematopoietic cell transplantation (HCT) have been improved by personalizing the doses to target narrow busulfan plasma exposure. An interlaboratory proficiency test program for the quantitation, pharmacokinetic modeling, and busulfan dosing in plasma was developed. Previous proficiency rounds (ie, the first 2) found that 67%-85% and 71%-88% of the dose recommendations were inaccurate, respectively.
Methods: A proficiency test scheme was developed by the Dutch Foundation for Quality Assessment in Medical Laboratories (SKML) and consisted of 2 rounds per year, with each round containing 2 busulfan samples. In this study, 5 subsequent proficiency tests were evaluated. In each round, the participating laboratories reported their results for 2 proficiency samples (ie, low and high busulfan concentrations) and a theoretical case assessing their pharmacokinetic modeling and dose recommendations. Descriptive statistics were performed, with ±15% for busulfan concentrations and ±10% for busulfan plasma exposure. The dose recommendations were deemed accurate.
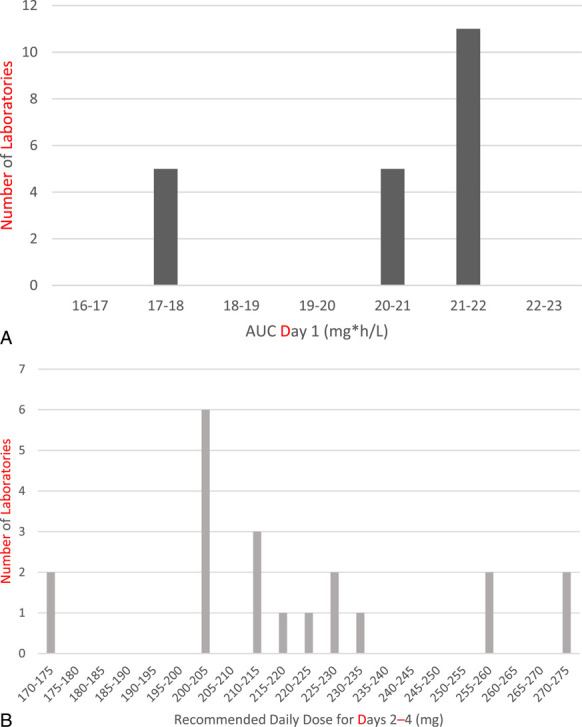
Results: Since January 2020, 41 laboratories have participated in at least 1 round of this proficiency test. Over the 5 rounds, an average of 78% of the busulfan concentrations were accurate. Area under the concentration-time curve calculations were accurate in 75%-80% of the cases, whereas only 60%-69% of the dose recommendations were accurate. Compared with the first 2 proficiency test rounds (PMID 33675302, October, 2021), the busulfan quantitation results were similar, but the dose recommendations worsened. Some laboratories repeatedly submit results that deviated by more than 15% from the reference values.
Conclusions: The proficiency test showed persistent inaccuracies in busulfan quantitation, pharmacokinetic modeling, and dose recommendations. Additional educational efforts have yet to be implemented; regulatory efforts seem to be needed. The use of specialized busulfan pharmacokinetic laboratories or a sufficient performance in busulfan proficiency tests should be required for HCT centers that prescribe busulfan.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Association of Therapeutic Drug Monitoring and Clinical Toxicology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Deeg HJ, Maris MB, Scott BL, et al. Optimization of allogeneic transplant conditioning: not the time for dogma. Leukemia. 2006;20:1701–1705. - PubMed
-
- Palmer J, McCune JS, Perales MA, et al. Personalizing busulfan-based conditioning: considerations from the American society for Blood and marrow transplantation practice guidelines committee. Biol Blood Marrow Transpl. 2016;22:1915–1925. - PubMed
-
- McCune JS, Gibbs JP, Slattery JT. Plasma concentration monitoring of busulfan: does it improve clinical outcome? Clin Pharmacokinet. 2000;39:155–165. - PubMed
-
- McCune JS, Holmberg LA. Busulfan in hematopoietic stem cell transplant setting. Expert Opin Drug Metab Toxicol. 2009;5:957–969. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
