

Post-Stroke Neuropsychiatric Complications: Types, Pathogenesis, and Therapeutic Intervention
- PMID: 37199575
- PMCID: PMC10676799
- DOI: 10.14336/AD.2023.0310-2
Post-Stroke Neuropsychiatric Complications: Types, Pathogenesis, and Therapeutic Intervention
Abstract
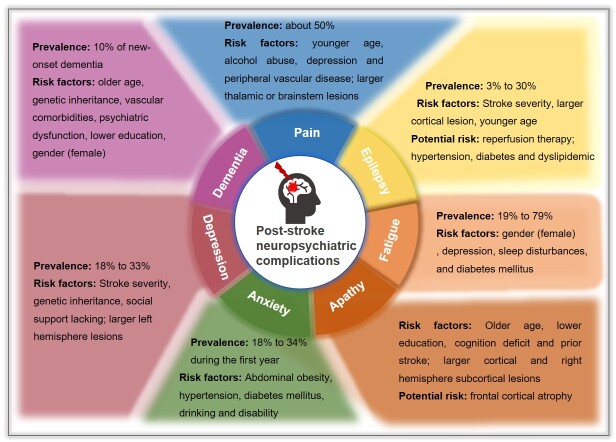
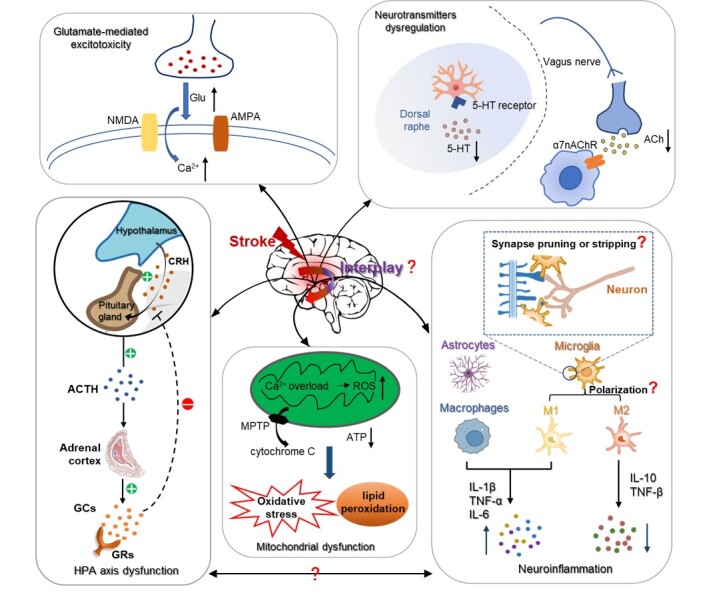
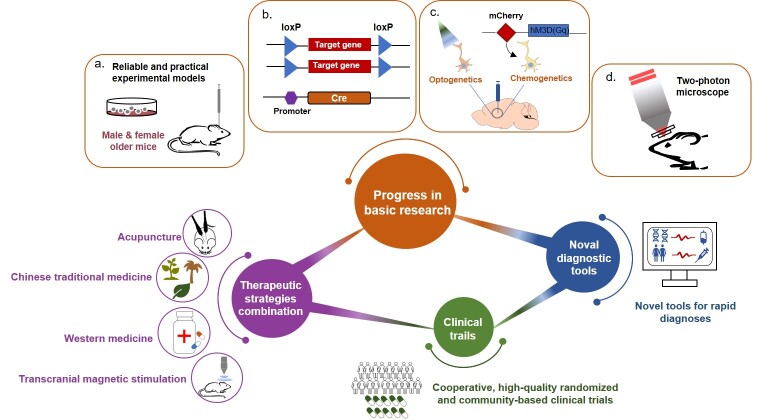
Almost all stroke survivors suffer physical disabilities and neuropsychiatric disturbances, which can be briefly divided into post-stroke neurological diseases and post-stroke psychiatric disorders. The former type mainly includes post-stroke pain, post-stroke epilepsy, and post-stroke dementia while the latter one includes post-stroke depression, post-stroke anxiety, post-stroke apathy and post-stroke fatigue. Multiple risk factors are related to these post-stroke neuropsychiatric complications, such as age, gender, lifestyle, stroke type, medication, lesion location, and comorbidities. Recent studies have revealed several critical mechanisms underlying these complications, namely inflammatory response, dysregulation of the hypothalamic pituitary adrenal axis, cholinergic dysfunction, reduced level of 5-hydroxytryptamine, glutamate-mediated excitotoxicity and mitochondrial dysfunction. Moreover, clinical efforts have successfully given birth to many practical pharmaceutic strategies, such as anti-inflammatory medications, acetylcholinesterase inhibitors, and selective serotonin reuptake inhibitors, as well as diverse rehabilitative modalities to help patients physically and mentally. However, the efficacy of these interventions is still under debate. Further investigations into these post-stroke neuropsychiatric complications, from both basic and clinical perspectives, are urgent for the development of effective treatment strategies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hankey GJ (2014). Secondary stroke prevention. Lancet Neurol, 13:178-194. - PubMed
-
- Ferro JM, Caeiro L, Figueira ML (2016). Neuropsychiatric sequelae of stroke. Nat Rev Neurol, 12:269-280. - PubMed
-
- Fornaro M, Solmi M, Veronese N, De Berardis D, Buonaguro EF, Tomasetti C, et al.. (2017). The burden of mood-disorder/cerebrovascular disease comorbidity: essential neurobiology, psychopharmacology, and physical activity interventions. Int Rev Psychiatry, 29:425-435. - PubMed
Publication types
LinkOut - more resources
Full Text Sources