

Neurocognitive outcomes in adult survivors of neuroblastoma: A report from the Childhood Cancer Survivor Study
- PMID: 37199722
- PMCID: PMC10523930
- DOI: 10.1002/cncr.34847
Neurocognitive outcomes in adult survivors of neuroblastoma: A report from the Childhood Cancer Survivor Study
Abstract
Background: Despite survival improvements, there is a paucity of data on neurocognitive outcomes in neuroblastoma survivors. This study addresses this literature gap.
Methods: Neurocognitive impairments in survivors were compared to sibling controls from the Childhood Cancer Survivor Study (CCSS) using the CCSS Neurocognitive Questionnaire. Impaired emotional regulation, organization, task efficiency, and memory defined as scores ≥90th percentile of sibling norms. Modified Poisson regression models evaluated associations with treatment exposures, era of diagnosis, and chronic conditions. Analyses were stratified by age at diagnosis (≤1 and >1 year) as proxy for lower versus higher risk disease.
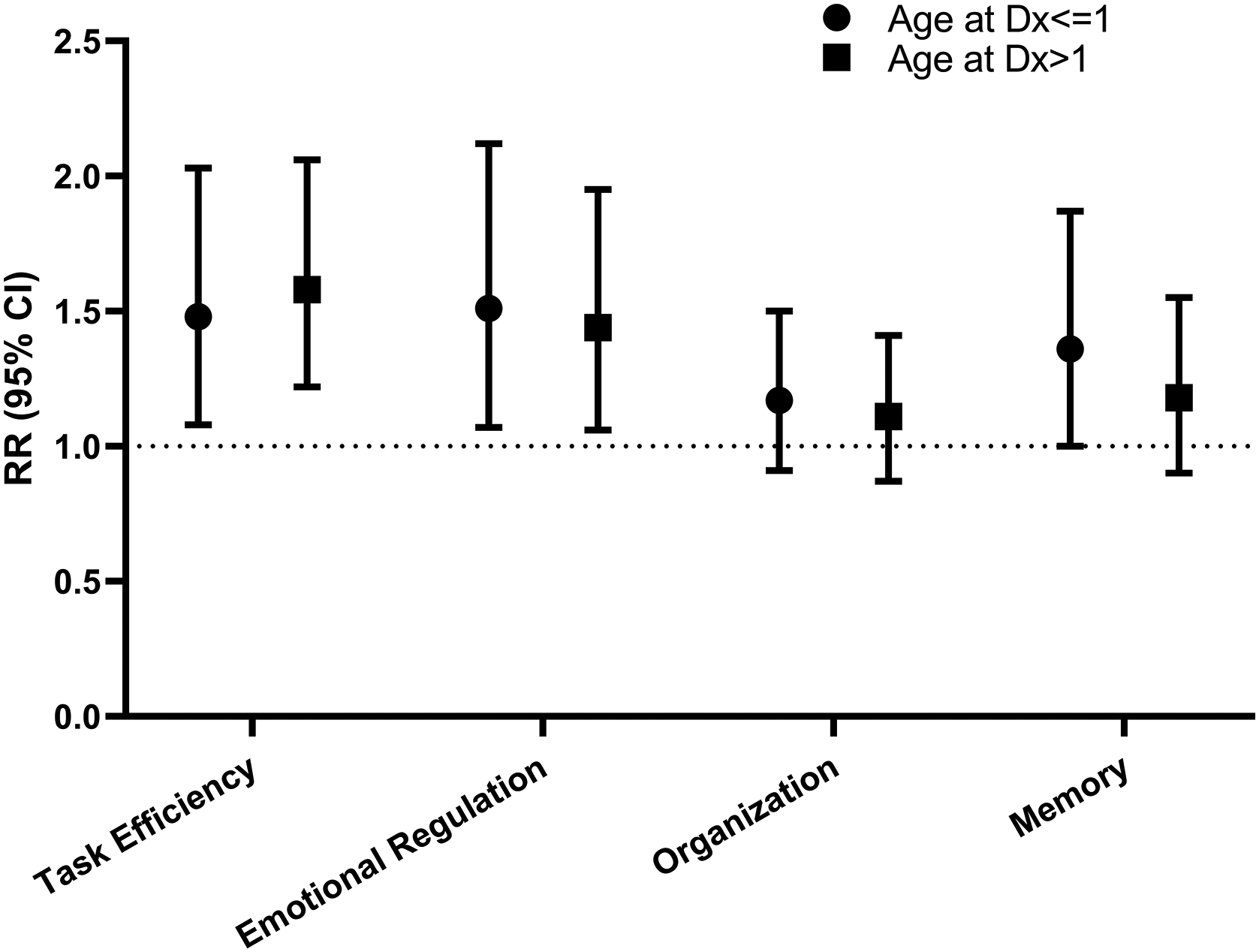
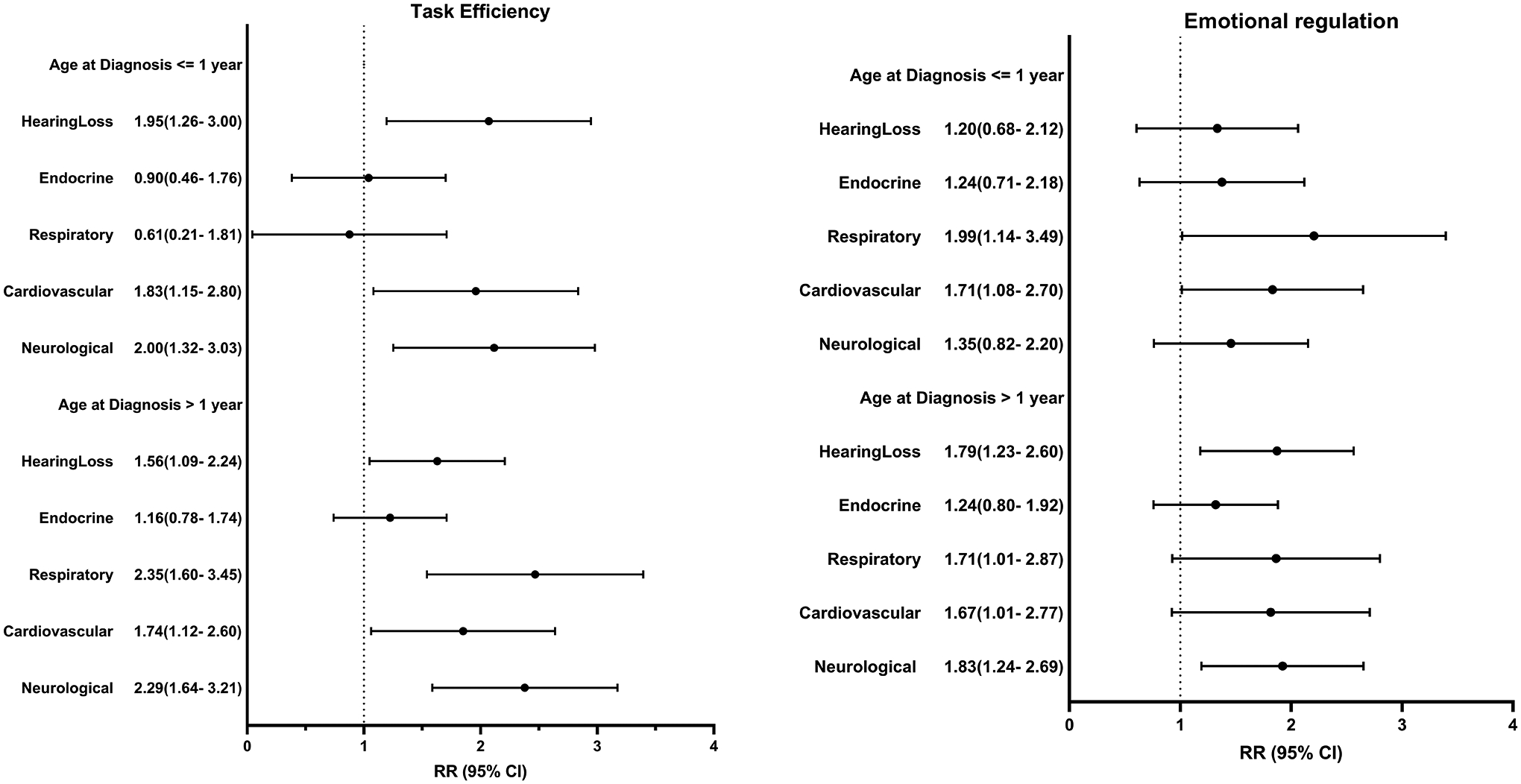
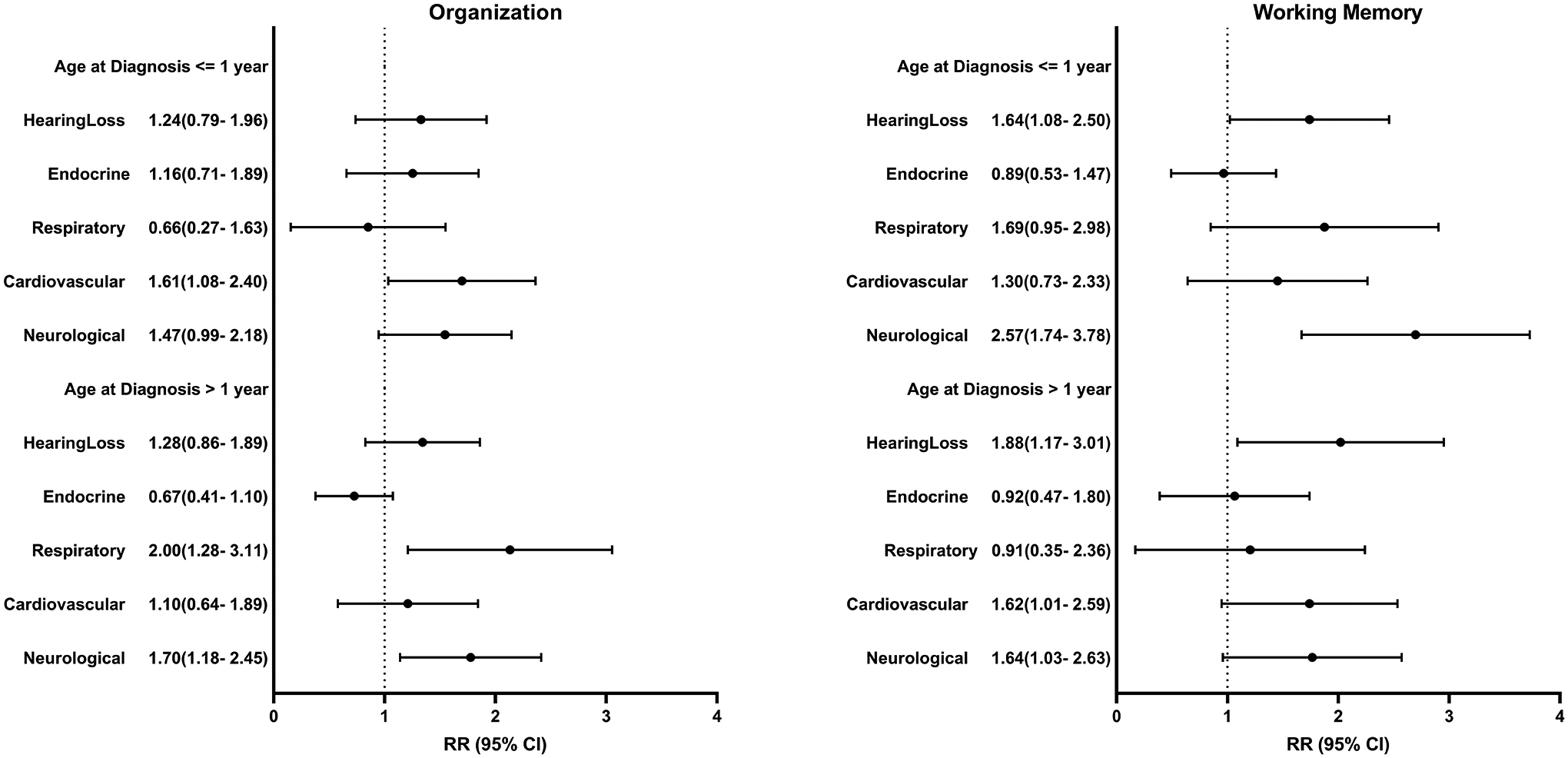
Results: Survivors (N = 837; median [range] age, 25 [17-58] years, age diagnosed, 1 [0-21] years) were compared to sibling controls (N = 728; age, 32 [16-43] years). Survivors had higher risk of impaired task efficiency (≤1 year relative risk [RR], 1.48; 95% confidence interval [CI], 1.08-2.03; >1 year RR, 1.58; 95% CI, 1.22-2.06) and emotional regulation (≤1 year RR, 1.51; 95% CI, 1.07-2.12; >1 year RR, 1.44; 95% CI, 1.06-1.95). Impaired task efficiency associated with platinum exposure (≤1 year RR, 1.74; 95% CI, 1.01-2.97), hearing loss (≤1 year RR, 1.95; 95% CI, 1.26-3.00; >1 year RR, 1.56; 95% CI, 1.09-2.24), cardiovascular (≤1 year RR, 1.83; 95% CI, 1.15-2.89; >1 year RR, 1.74; 95% CI, 1.12-2.69), neurologic (≤1 year RR, 2.00; 95% CI, 1.32-3.03; >1 year RR, 2.29; 95% CI, 1.64-3.21), and respiratory (>1 year RR, 2.35; 95% CI, 1.60-3.45) conditions. Survivors ≤1 year; female sex (RR, 1.54; 95% CI, 1.02-2.33), cardiovascular (RR, 1.71; 95% CI, 1.08-2.70) and respiratory (RR, 1.99; 95% CI, 1.14-3.49) conditions associated impaired emotional regulation. Survivors were less likely to be employed full-time (p < .0001), graduate college (p = .035), and live independently (p < .0001).
Conclusions: Neuroblastoma survivors report neurocognitive impairment impacting adult milestones. Identified health conditions and treatment exposures can be targeted to improve outcomes.
Plain language summary: Survival rates continue to improve in patients with neuroblastoma. There is a lack of information regarding neurocognitive outcomes in neuroblastoma survivors; most studies examined survivors of leukemia or brain tumors. In this study, 837 adult survivors of childhood neuroblastoma were compared to siblings from the Childhood Cancer Survivorship Study. Survivors had a 50% higher risk of impairment with attention/processing speed (task efficiency) and emotional reactivity/frustration tolerance (emotional regulation). Survivors were less likely to reach adult milestones such as living independently. Survivors with chronic health conditions are at a higher risk of impairment. Early identification and aggressive management of chronic conditions may help mitigate the level of impairment.
Keywords: Childhood Cancer Survivor Study; cancer survivor; neuroblastoma; neurocognitive.
© 2023 The Authors. Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
Figures
References
-
- DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64: 252–271. - PubMed
-
- Park JR, Bagatell R, London WB, et al. Children’s Oncology Group’s 2013 blueprint for research: neuroblastoma. Pediatr Blood Cancer. 2013;60: 985–993. - PubMed
-
- Evans AE. Treatment of neuroblastoma. Cancer. 1972;30: 1595–1599. - PubMed
-
- Matthay KK, Villablanca JG, Seeger RC, et al. Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation, and 13-cis-retinoic acid. Children’s Cancer Group. N Engl J Med. 1999;341: 1165–1173. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
