

Scapho-luno-capitate fusion with proximal lunate articular surface preservation for management of grade IIIA Kienböck's disease: a prospective case series
- PMID: 37199858
- PMCID: PMC10195948
- DOI: 10.1186/s10195-023-00703-9
Scapho-luno-capitate fusion with proximal lunate articular surface preservation for management of grade IIIA Kienböck's disease: a prospective case series
Abstract
Background: Kienböck's disease is idiopathic lunate avascular necrosis, which may lead to lunate collapse, abnormal carpal motion and wrist arthritis. The current study aimed to assess the outcomes of treating stage IIIA Kienböck's disease by a novel technique of limited carpal fusion via partial lunate excision with preservation of the proximal lunate surface and scapho-luno-capitate (SLC) fusion.
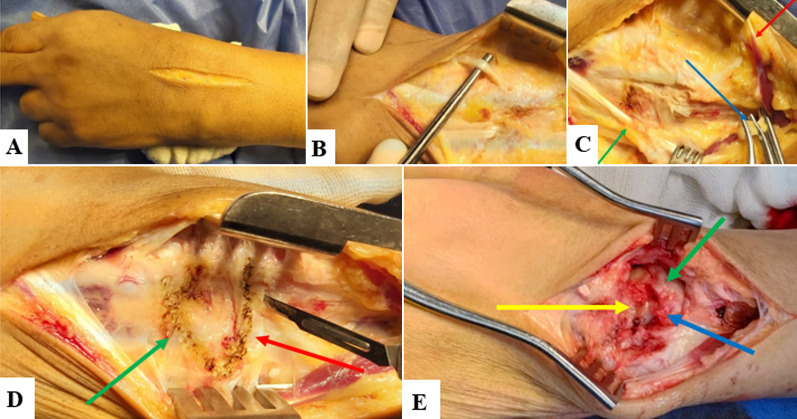
Materials and methods: We conducted a prospective study of patients with grade IIIA Kienböck's disease managed with a novel technique of limited carpal fusion comprising SLC fusion with preservation of the proximal lunate articular cartilage. Autologous iliac crest bone grafting and K-wires fixation were used to enhance the osteosynthesis of the SLC fusion. The minimum follow-up period was 1 year. A visual analog scale (VAS) and the Mayo Wrist Score were utilized for the evaluation of patient residual pain and functional assessment, respectively. A digital Smedley dynamometer was used to measure the grip strength. The modified carpal height ratio (MCHR) was used for monitoring carpal collapse. The radioscaphoid angle, scapholunate angle, and the modified carpal-ulnar distance ratio were used for the assessment of carpal bones alignment and ulnar translocation of carpal bones.
Results: This study included 20 patients with a mean age of 27.9 ± 5.5 years. At the last follow-up, the mean range of flexion/extension range of motion (% of normal side) improved from 52.8 ± 5.4% to 65.7 ± 11.1%, P = 0.002, the mean grip strength (% of normal side) improved from 54.6 ± 11.8% to 88.3 ± 12.4%, P = 0.001, the mean Mayo Wrist Score improved from 41.5 ± 8.2 to 81 ± 9.2, P = 0.002, and the mean VAS score reduced from 6.1 ± 1.6 to 0.6 ± 0.4, P = 0.004. The mean follow-up MCHR improved from 1.46 ± 0.11 to 1.59 ± 0.34, P = 0.112. The mean radioscaphoid angle improved from 63 ± 10º to 49 ± 6º, P = 0.011. The mean scapholunate angle increased from 32 ± 6º to 47 ± 8º, P = 0.004. The mean modified carpal-ulnar distance ratio was preserved and none of the patients developed ulnar translocation of the carpal bones. Radiological union was achieved in all patients.
Conclusions: Scapho-luno-capitate fusion with partial lunate excision and preservation of the proximal lunate surface is a valuable option for treating stage IIIA Kienböck's disease, with satisfactory outcomes. Level of evidence Level IV. Trial registration Not applicable.
Keywords: Iliac crest graft; K-wires; Kienböck’s disease; Limited carpal fusion; Lunate avascular necrosis; Scapho-luno-capitate fusion.
© 2023. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures

Similar articles
-
Treatment of Kienböck's Disease With Neutral Ulnar Variance by Distal Capitate Shortening and Arthrodesis to the Base of the Third Metacarpal Bone.J Hand Surg Am. 2019 Jun;44(6):518.e1-518.e9. doi: 10.1016/j.jhsa.2018.08.010. Epub 2018 Oct 8. J Hand Surg Am. 2019. PMID: 30309665
-
Examining the Efficacy of Arthroscopic Scaphocapitate Arthrodesis for Advanced Kienbock's Disease: Clinical and Radiological Outcomes.Clin Orthop Surg. 2024 Jun;16(3):448-454. doi: 10.4055/cios23167. Epub 2024 Apr 8. Clin Orthop Surg. 2024. PMID: 38827751 Free PMC article.
-
Capitate shortening osteotomy with or without vascularized bone grafting for the treatment of early stages of Kienböck's disease.Int Orthop. 2021 Oct;45(10):2635-2641. doi: 10.1007/s00264-021-05103-4. Epub 2021 Jul 15. Int Orthop. 2021. PMID: 34264352
-
Scaphocapitate fusion for the treatment of Lichtman stage III Kienböck's disease. Results of a single center study with literature review.Hand Surg Rehabil. 2020 May;39(3):201-206. doi: 10.1016/j.hansur.2020.01.002. Epub 2020 Feb 15. Hand Surg Rehabil. 2020. PMID: 32070792 Review.
-
Arthroscopic assessment and classification of Kienbock's disease.Tech Hand Up Extrem Surg. 2006 Mar;10(1):8-13. doi: 10.1097/00130911-200603000-00003. Tech Hand Up Extrem Surg. 2006. PMID: 16628114 Review.
Cited by
-
Lunate bone excision and scaphocapitate arthrodesis in late stages of Kienböck's disease: a long-term prospective study.Int Orthop. 2025 May;49(5):1143-1152. doi: 10.1007/s00264-025-06458-8. Epub 2025 Mar 1. Int Orthop. 2025. PMID: 40024945 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
