

Long-Term Efficacy and Safety of Upadacitinib in Patients with Rheumatoid Arthritis: Final Results from the BALANCE-EXTEND Open-Label Extension Study
- PMID: 37199884
- PMCID: PMC10193312
- DOI: 10.1007/s40744-023-00557-x
Long-Term Efficacy and Safety of Upadacitinib in Patients with Rheumatoid Arthritis: Final Results from the BALANCE-EXTEND Open-Label Extension Study
Abstract
Introduction: Upadacitinib (UPA) is an oral, selective Janus kinase inhibitor that has demonstrated favorable efficacy with an acceptable safety profile across a global, phase 3 program in rheumatoid arthritis (RA). This phase 2 open-label extension investigated the efficacy and safety of UPA through 6 years of treatment.
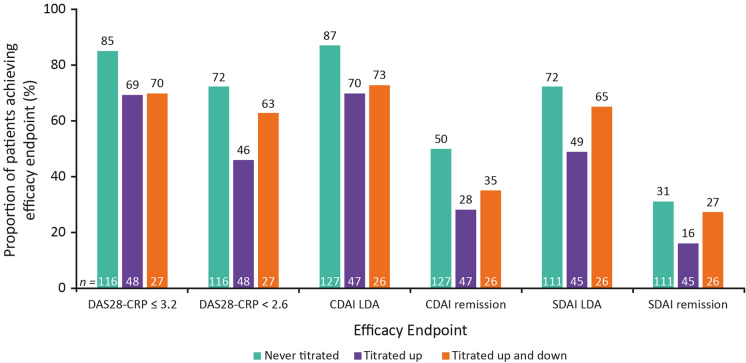
Methods: Patients from two phase 2b trials (BALANCE-1 and -2) enrolled in BALANCE-EXTEND (NCT02049138) and received open-label UPA 6 mg twice daily (BID). Dose increases to 12 mg BID were required for patients with < 20% improvement in swollen or tender joint counts at weeks 6 or 12 and permitted for those not achieving Clinical Disease Activity Index (CDAI) low disease activity (LDA; CDAI 2.8 to ≤ 10). Dose reduction to UPA 6 mg BID was permitted only for safety or tolerability reasons. After January 2017, the 6/12 mg BID doses were replaced by 15/30 mg once-daily extended-release equivalents. Efficacy and safety were monitored up to 6 years of UPA treatment; outcomes included rates of achievement of LDA or remission. Data were analyzed for patients who received the lower UPA dose throughout; titrated up to the higher UPA dose from weeks 6 or 12; or titrated to the higher UPA dose and back down.
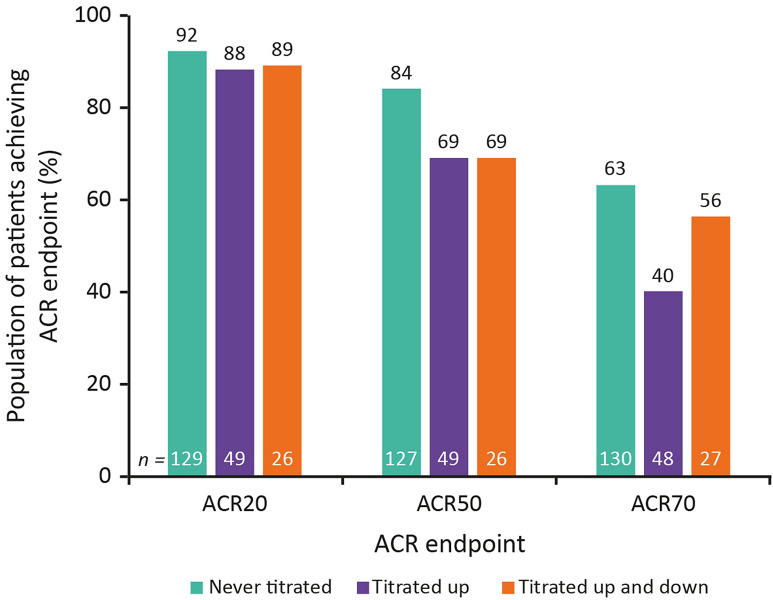
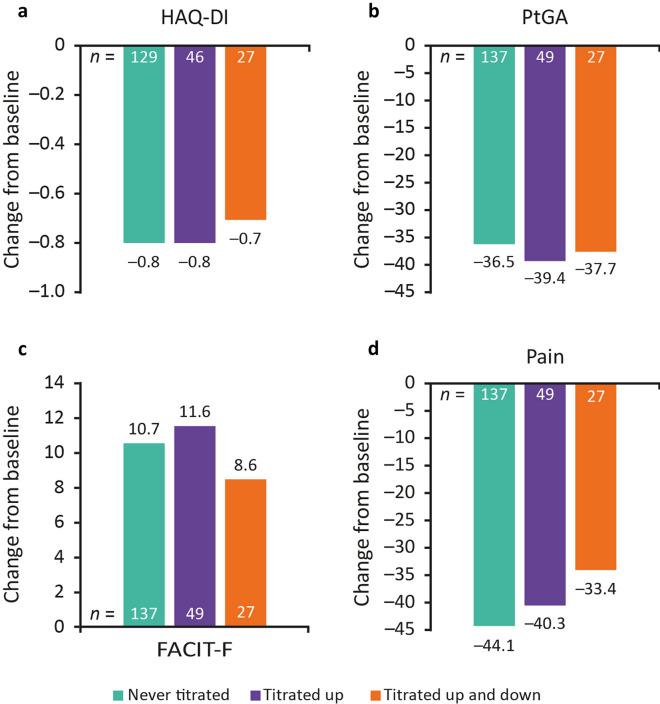
Results: Overall, 493 patients entered BALANCE-EXTEND ('Never titrated', n = 306; 'Titrated up', n = 149; 'Titrated up and down', n = 38), and 223 patients (45%) completed the 6-year study. Total cumulative exposure was 1863 patient-years. Rates of LDA and remission were maintained through 6 years. Overall, 87%/70%/73% of patients in the 'Never titrated'/'Titrated up'/'Titrated up and down' groups achieved CDAI LDA at week 312, while the respective rates of Disease Activity Score 28 with C-reactive protein meeting LDA and remission criteria were 85%/69%/70% and 72%/46%/63%. Improvements in patient-reported outcomes were similar among the three groups. No new safety signals were identified.
Conclusions: In this open-label extension of two phase 2 studies, UPA demonstrated sustained efficacy and an acceptable safety profile through 6 years of treatment in patients who completed the study. These data support a favorable long-term benefit-risk profile of UPA in patients with RA.
Trial registration: Trial registration number: NCT02049138.
Keywords: Extension; Janus kinase inhibitor; Phase 3; Rheumatoid arthritis; Treatment; Upadacitinib.
© 2023. The Author(s).
Conflict of interest statement
Alan Kivitz has received consulting fees and/or honoraria from AbbVie, Amgen, Boehringer Ingelheim, Celgene Corporation, EcoR1 Capital, Flexion Therapeutics, Genentech, Gilead, GlaxoSmithKline, Grünenthal, Horizon, Janssen, Lilly, Merck, Novartis, Orion, Pfizer, Regeneron Pharmaceuticals, SUN Pharma Advanced Research, and UCB; owns stocks or options in Amgen, Gilead, GlaxoSmithKline, Novartis, Pfizer, and Sanofi; has received fees from AbbVie for his role as a Principal Investigator in the study; and is a board and/or advisory board member for AbbVie, Bendcare LLC, Boehringer Ingelheim, ChemoCentryx, Flexion, Gilead, Grünenthal, Horizon, Janssen, Lilly, Novartis, Pfizer, Regeneron, and UCB. Alvin F. Wells has received consulting fees and research support from AbbVie. Juan I. Vargas has received honoraria and fees from AbbVie as a Principal Investigator in the study. Herbert S. B. Baraf has received grant/research support from AbbVie, Genentech, Gilead, Janssen, and Lilly; has acted as a consultant for Gilead and Janssen; and has received honoraria and fees from AbbVie as a Principal Investigator in the study. He has retired from the Center for Rheumatology and Bone Research since the completion of the study. Maureen Rischmueller has received grant/research support from AbbVie, Amgen, BMS, Janssen Global Services, Lilly, Novartis, Pfizer, Sanofi Pasteur Biologics, and UCB Biosciences; and has acted as a consultant for AbbVie, BMS, CSL Behring, Gilead, Janssen Global Services, Lilly, Pfizer, Sanofi US Services, and UCB Biosciences. Justin Klaff, Nasser Khan, Yihan Li, Kyle Carter, and Alan Friedman are employees of AbbVie and may own stocks or options. Patrick Durez has received speaker fees from AbbVie, Galapagos, Lilly, Nordimed, and Thermo Fisher Scientific Inc.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
