

Incidence and Outcomes of Non-Ventilator-Associated Hospital-Acquired Pneumonia in 284 US Hospitals Using Electronic Surveillance Criteria
- PMID: 37200031
- PMCID: PMC10196873
- DOI: 10.1001/jamanetworkopen.2023.14185
Incidence and Outcomes of Non-Ventilator-Associated Hospital-Acquired Pneumonia in 284 US Hospitals Using Electronic Surveillance Criteria
Abstract
Importance: Non-ventilator-associated hospital-acquired pneumonia (NV-HAP) is a common and deadly hospital-acquired infection. However, inconsistent surveillance methods and unclear estimates of attributable mortality challenge prevention.
Objective: To estimate the incidence, variability, outcomes, and population attributable mortality of NV-HAP.
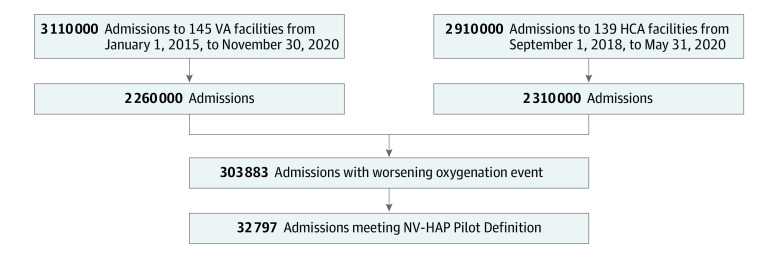
Design, setting, and participants: This cohort study retrospectively applied clinical surveillance criteria for NV-HAP to electronic health record data from 284 US hospitals. Adult patients admitted to the Veterans Health Administration hospital from 2015 to 2020 and HCA Healthcare hospitals from 2018 to 2020 were included. The medical records of 250 patients who met the surveillance criteria were reviewed for accuracy.
Exposures: NV-HAP, defined as sustained deterioration in oxygenation for 2 or more days in a patient who was not ventilated concurrent with abnormal temperature or white blood cell count, performance of chest imaging, and 3 or more days of new antibiotics.
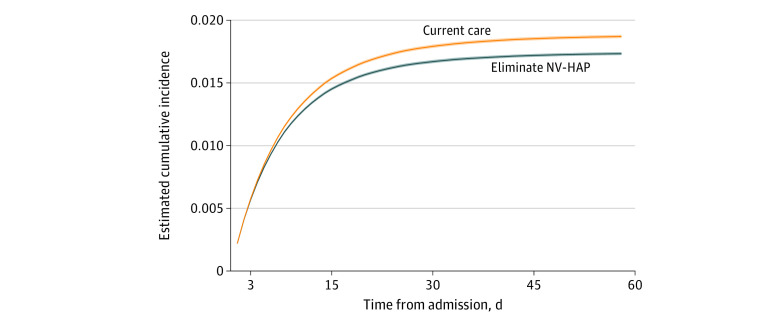
Main outcomes and measures: NV-HAP incidence, length-of-stay, and crude inpatient mortality. Attributable inpatient mortality by 60 days follow-up was estimated using inverse probability weighting, accounting for both baseline and time-varying confounding.
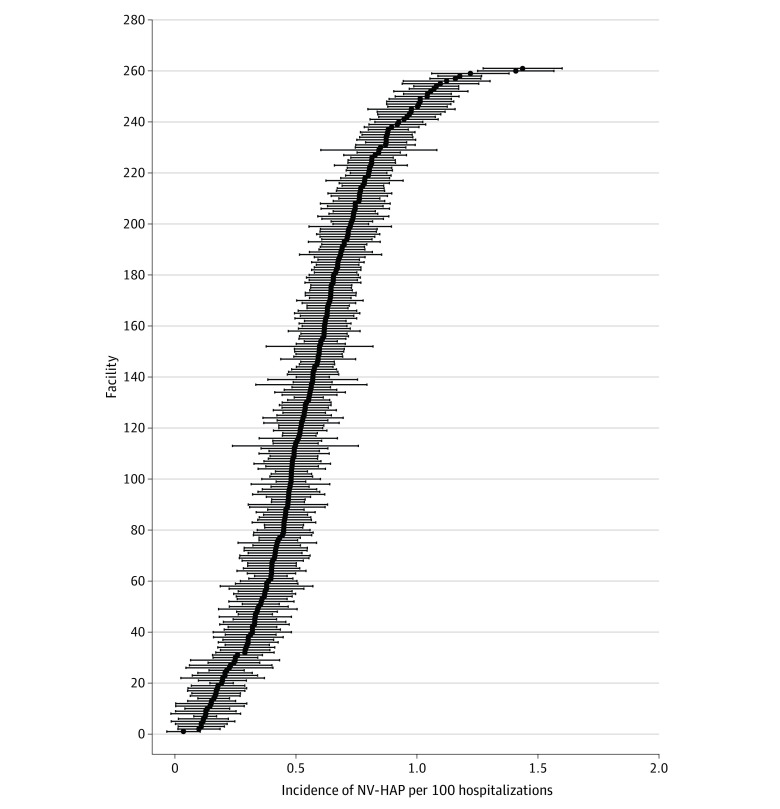
Results: Among 6 022 185 hospitalizations (median [IQR] age, 66 [54-75] years; 1 829 475 [26.1%] female), there were 32 797 NV-HAP events (0.55 per 100 admissions [95% CI, 0.54-0.55] per 100 admissions and 0.96 per 1000 patient-days [95% CI, 0.95-0.97] per 1000 patient-days). Patients with NV-HAP had multiple comorbidities (median [IQR], 6 [4-7]), including congestive heart failure (9680 [29.5%]), neurologic conditions (8255 [25.2%]), chronic lung disease (6439 [19.6%]), and cancer (5,467 [16.7%]); 24 568 cases (74.9%) occurred outside intensive care units. Crude inpatient mortality was 22.4% (7361 of 32 797) for NV-HAP vs 1.9% (115 530 of 6 022 185) for all hospitalizations; 12 449 (8.0%) were discharged to hospice. Median [IQR] length-of-stay was 16 (11-26) days vs 4 (3-6) days. On medical record review, pneumonia was confirmed by reviewers or bedside clinicians in 202 of 250 patients (81%). It was estimated that NV-HAP accounted for 7.3% (95% CI, 7.1%-7.5%) of all hospital deaths (total hospital population inpatient death risk of 1.87% with NV-HAP events included vs 1.73% with NV-HAP events excluded; risk ratio, 0.927; 95% CI, 0.925-0.929).
Conclusions and relevance: In this cohort study, NV-HAP, which was defined using electronic surveillance criteria, was present in approximately 1 in 200 hospitalizations, of whom 1 in 5 died in the hospital. NV-HAP may account for up to 7% of all hospital deaths. These findings underscore the need to systematically monitor NV-HAP, define best practices for prevention, and track their impact.
Conflict of interest statement
Figures
Similar articles
-
Development and Assessment of Objective Surveillance Definitions for Nonventilator Hospital-Acquired Pneumonia.JAMA Netw Open. 2019 Oct 2;2(10):e1913674. doi: 10.1001/jamanetworkopen.2019.13674. JAMA Netw Open. 2019. PMID: 31626321 Free PMC article.
-
The association between non-ventilator associated hospital acquired pneumonia and patient outcomes among U.S. Veterans.Am J Infect Control. 2022 Dec;50(12):1339-1345. doi: 10.1016/j.ajic.2022.02.023. Epub 2022 Feb 26. Am J Infect Control. 2022. PMID: 35231564
-
Electronic surveillance criteria for non-ventilator-associated hospital-acquired pneumonia: Assessment of reliability and validity.Infect Control Hosp Epidemiol. 2023 Mar 15:1-7. doi: 10.1017/ice.2022.302. Online ahead of print. Infect Control Hosp Epidemiol. 2023. PMID: 36920040
-
Clinical utility of telavancin for treatment of hospital-acquired pneumonia: focus on non-ventilator-associated pneumonia.Infect Drug Resist. 2014 May 20;7:129-35. doi: 10.2147/IDR.S25930. eCollection 2014. Infect Drug Resist. 2014. PMID: 24876786 Free PMC article. Review.
-
Practices to prevent non-ventilator hospital-acquired pneumonia: a narrative review.J Hosp Infect. 2024 Sep;151:201-212. doi: 10.1016/j.jhin.2024.03.019. Epub 2024 Apr 23. J Hosp Infect. 2024. PMID: 38663517 Review.
Cited by
-
Comparison of the end-of-life decisions of patients with hospital-acquired pneumonia after the enforcement of the life-sustaining treatment decision act in Korea.BMC Med Ethics. 2023 Jul 18;24(1):52. doi: 10.1186/s12910-023-00931-y. BMC Med Ethics. 2023. PMID: 37461075 Free PMC article.
-
Stewardship Prompts to Improve Antibiotic Selection for Pneumonia: The INSPIRE Randomized Clinical Trial.JAMA. 2024 Jun 18;331(23):2007-2017. doi: 10.1001/jama.2024.6248. JAMA. 2024. PMID: 38639729 Free PMC article. Clinical Trial.
-
Implementation of a structured oral hygiene program through nursing assistant education to address non-ventilator hospital-acquired pneumonia: A quasi-experimental study.J Nurs Scholarsh. 2025 Mar;57(2):204-215. doi: 10.1111/jnu.13018. Epub 2024 Aug 26. J Nurs Scholarsh. 2025. PMID: 39185740 Free PMC article.
-
Automated surveillance of non-ventilator-associated hospital-acquired pneumonia (nvHAP): a systematic literature review.Antimicrob Resist Infect Control. 2024 Mar 6;13(1):30. doi: 10.1186/s13756-024-01375-8. Antimicrob Resist Infect Control. 2024. PMID: 38449045 Free PMC article.
-
Effect of nutritional status on occurrence of pneumonia after traumatic cervical spinal cord injury.Sci Rep. 2024 Jun 10;14(1):13286. doi: 10.1038/s41598-024-64121-5. Sci Rep. 2024. PMID: 38858459 Free PMC article.
References
-
- Cassini A, Plachouras D, Eckmanns T, et al. . Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016;13(10):e1002150. doi:10.1371/journal.pmed.1002150 - DOI - PMC - PubMed
-
- Zilberberg MD, Nathanson BH, Puzniak LA, Shorr AF. Descriptive epidemiology and outcomes of nonventilated hospital-acquired, ventilated hospital-acquired, and ventilator-associated bacterial pneumonia in the United States, 2012-2019. Crit Care Med. 2022;50(3):460-468. doi:10.1097/CCM.0000000000005298 - DOI - PMC - PubMed
-
- National Healthcare Safety Network. Pneumonia (ventilator-associated [VAP] and non–ventilator-associated Pneumonia [PNEU]) event. US Centers for Disease Control and Prevention. Accessed April 13, 2023. https://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
