

Potential Clinical and Economic Outcomes of Over-the-Counter Hearing Aids in the US
- PMID: 37200042
- PMCID: PMC10196927
- DOI: 10.1001/jamaoto.2023.0949
Potential Clinical and Economic Outcomes of Over-the-Counter Hearing Aids in the US
Abstract
Importance: Over-the-counter (OTC) hearing aids are now available in the US; however, their clinical and economic outcomes are unknown.
Objective: To project the clinical and economic outcomes of traditional hearing aid provision compared with OTC hearing aid provision.
Design, setting, and participants: This cost-effectiveness analysis used a previously validated decision model of hearing loss (HL) to simulate US adults aged 40 years and older across their lifetime in US primary care offices who experienced yearly probabilities of acquiring HL (0.1%-10.4%), worsening of their HL, and traditional hearing aid uptake (0.5%-8.1%/y at a fixed uptake cost of $3690) and utility benefits (0.11 additional utils/y). For OTC hearing aid provision, persons with perceived mild to moderate HL experienced increased OTC hearing aid uptake (1%-16%/y) based on estimates of time to first HL diagnosis. In the base case, OTC hearing aid utility benefits ranged from 0.05 to 0.11 additional utils/y (45%-100% of traditional hearing aids), and costs were $200 to $1400 (5%-38% of traditional hearing aids). Distributions were assigned to parameters to conduct probabilistic uncertainty analysis.
Intervention: Provision of OTC hearing aids, at increased uptake rates, across a range of effectiveness and costs.
Main outcomes and measures: Lifetime undiscounted and discounted (3%/y) costs and quality-adjusted life-years (QALYs) and incremental cost-effectiveness ratios (ICERs).
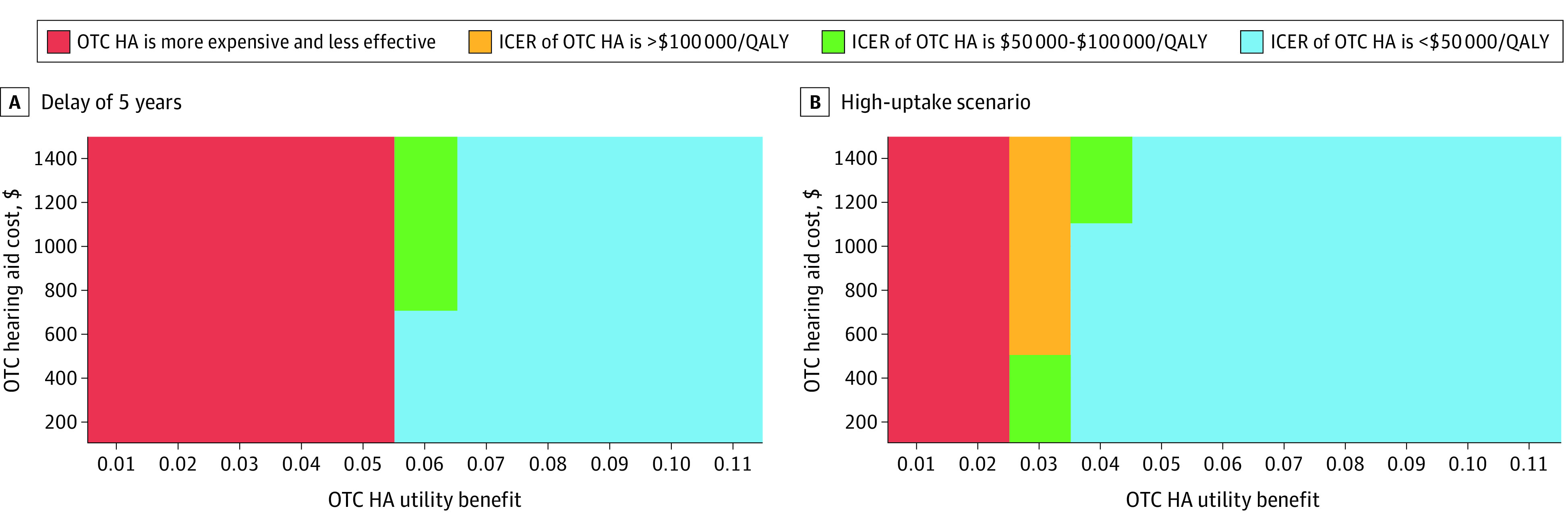
Results: Traditional hearing aid provision resulted in 18.162 QALYs, compared with 18.162 to 18.186 for OTC hearing aids varying with OTC hearing aid utility benefit (45%-100% that of traditional hearing aids). Provision of OTC hearing aids was associated with greater lifetime discounted costs by $70 to $200 along with OTC device cost ($200-$1000/pair; 5%-38% traditional hearing aid cost) due to increased hearing aid uptake. Provision of OTC hearing aids was considered cost-effective (ICER<$100 000/QALY) if the OTC utility benefit was 0.06 or greater (55% of the traditional hearing aid effectiveness). In probabilistic uncertainty analysis, OTC hearing aid provision was cost-effective in 53% of simulations.
Conclusions and relevance: In this cost-effectiveness analysis, provision of OTC hearing aids was associated with greater uptake of hearing intervention and was cost-effective over a range of prices so long as OTC hearing aids were greater than 55% as beneficial to patient quality of life as traditional hearing aids.
Conflict of interest statement
Figures

References
-
- World Health Organization . World report on hearing. Published March 3, 2021. Accessed February 17, 2022. https://www.who.int/publications/i/item/9789240020481
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
