

Stratified Simple Random Sampling Versus Volunteer Community-Wide Sampling for Estimates of COVID-19 Prevalence
- PMID: 37200600
- PMCID: PMC10262242
- DOI: 10.2105/AJPH.2023.307303
Stratified Simple Random Sampling Versus Volunteer Community-Wide Sampling for Estimates of COVID-19 Prevalence
Abstract
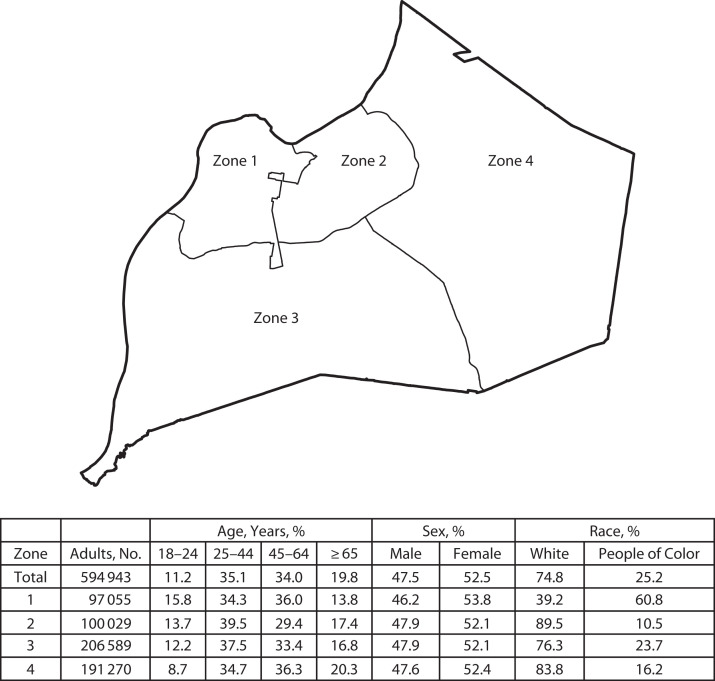
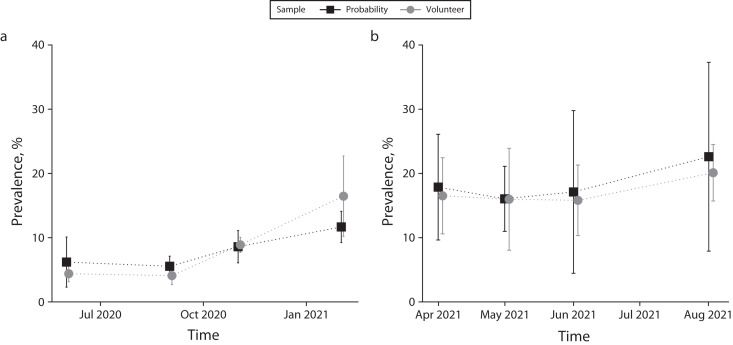
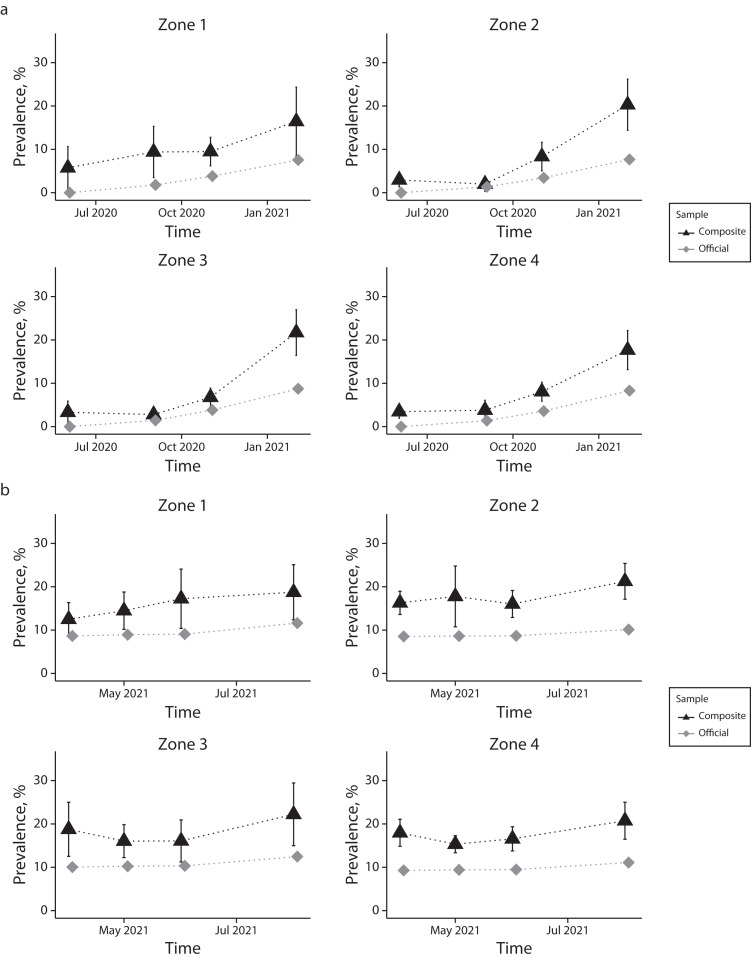
Objectives. To evaluate community-wide prevalence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection using stratified simple random sampling. Methods. We obtained data for the prevalence of SARS-CoV-2 in Jefferson County, Kentucky, from adult random (n = 7296) and volunteer (n = 7919) sampling over 8 waves from June 2020 through August 2021. We compared results with administratively reported rates of COVID-19. Results. Randomized and volunteer samples produced equivalent prevalence estimates (P < .001), which exceeded the administratively reported rates of prevalence. Differences between them decreased as time passed, likely because of seroprevalence temporal detection limitations. Conclusions. Structured targeted sampling for seropositivity against SARS-CoV-2, randomized or voluntary, provided better estimates of prevalence than administrative estimates based on incident disease. A low response rate to stratified simple random sampling may produce quantified disease prevalence estimates similar to a volunteer sample. Public Health Implications. Randomized targeted and invited sampling approaches provided better estimates of disease prevalence than administratively reported data. Cost and time permitting, targeted sampling is a superior modality for estimating community-wide prevalence of infectious disease, especially among Black individuals and those living in disadvantaged neighborhoods. (Am J Public Health. 2023;113(7):768-777. https://doi.org/10.2105/AJPH.2023.307303).
Figures
Comment in
-
Probability Samples Provide a Means of Benchmarking and Adjusting for Data Collected From Nonprobability Samples.Am J Public Health. 2023 Jul;113(7):721-723. doi: 10.2105/AJPH.2023.307317. Am J Public Health. 2023. PMID: 37285564 Free PMC article. No abstract available.
References
-
- Snow J. Mode of Communication of Cholera. 2nd ed. London, England: John Churchill; 1855.
-
- Hultsch DF, MacDonald SW, Hunter MA, Maitland SB, Dixon RA. Sampling and generalisability in developmental research: comparison of random and convenience samples of older adults. Int J Behav Dev. 2002;26(4):345–359. doi: 10.1080/01650250143000247. - DOI
-
- Kelly H, Riddell MA, Gidding HF, Nolan T, Gilbert GL. A random cluster survey and a convenience sample give comparable estimates of immunity to vaccine preventable diseases in children of school age in Victoria, Australia. Vaccine. 2002;20(25–26):3130–3136. doi: 10.1016/S0264-410X(02)00255-4. - DOI - PubMed
-
- Cheung KL, Peter M, Smit C, de Vries H, Pieterse ME. The impact of non-response bias due to sampling in public health studies: a comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health. 2017;17(1):276. doi: 10.1186/s12889-017-4189-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
