

Bictegravir/emtricitabine/tenofovir alafenamide as initial treatment for HIV-1: five-year follow-up from two randomized trials
- PMID: 37200995
- PMCID: PMC10186485
- DOI: 10.1016/j.eclinm.2023.101991
Bictegravir/emtricitabine/tenofovir alafenamide as initial treatment for HIV-1: five-year follow-up from two randomized trials
Abstract
Background: Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) is a single-tablet regimen recommended for HIV-1 treatment. The safety and efficacy of B/F/TAF as initial therapy was established in two Phase 3 studies: 1489 (vs dolutegravir [DTG]/abacavir/lamivudine) and 1490 (vs DTG + F/TAF). After 144 weeks of randomized follow-up, an open-label extension evaluated B/F/TAF to 240 weeks.
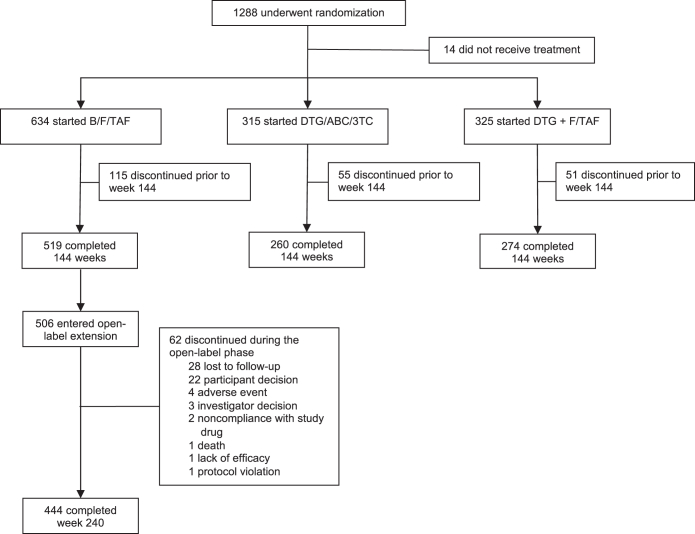
Methods: Of 634 participants randomized to B/F/TAF, 519 completed the double-blinded treatment, and 506/634 (80%) chose the 96-week open-label B/F/TAF extension, which was completed by 444/506 (88%) participants. Efficacy was based on the secondary outcome of the proportion of participants with HIV-1 RNA <50 copies/mL at Week 240 by missing = excluded and missing = failure methods. All 634 participants who were randomized to B/F/TAF and received at least one dose of B/F/TAF were included in efficacy and safety analyses. (Study 1489: ClinicalTrials.govNCT02607930; EudraCT 2015-004024-54. Study 1490: ClinicalTrials.govNCT02607956; EudraCT 2015-003988-10).
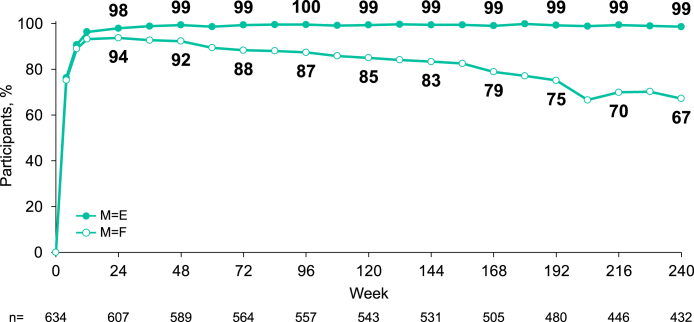
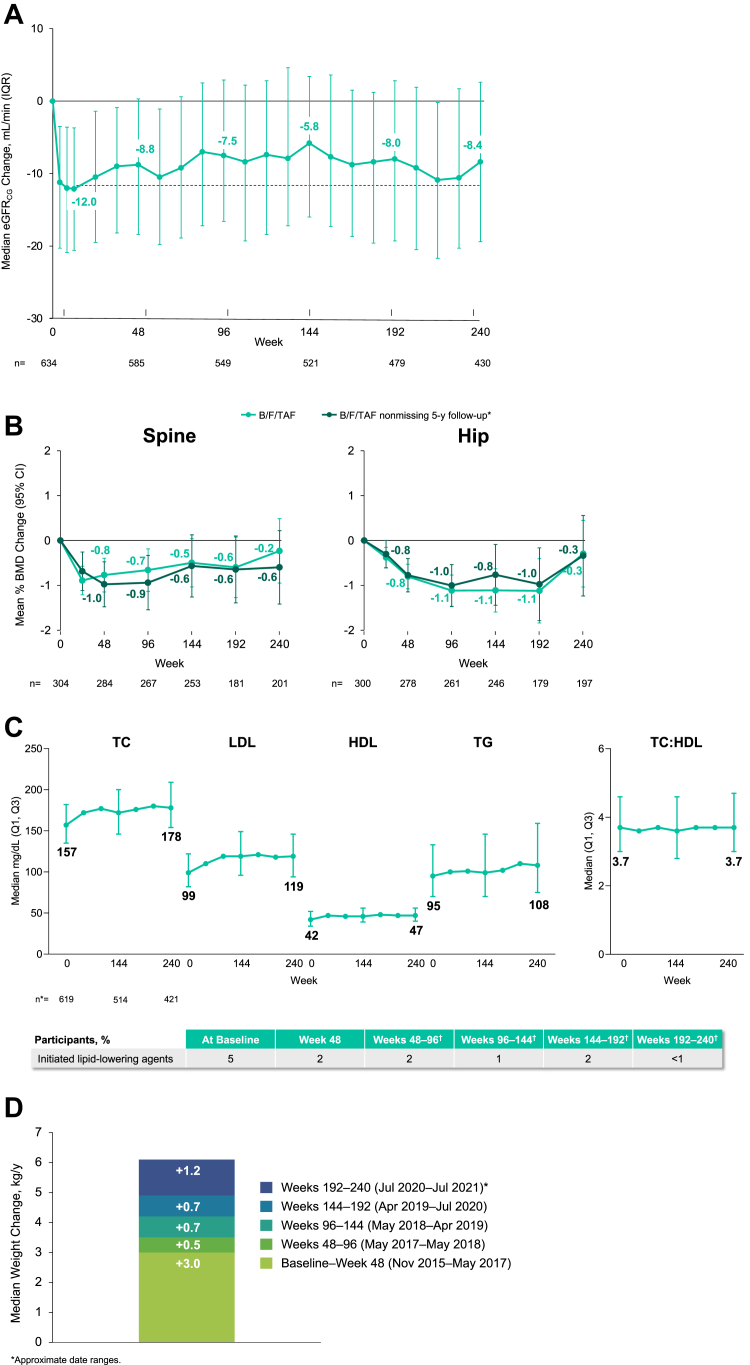
Findings: Of those with available virologic data, 98.6% (95% CI [97.0%-99.5%], 426/432) maintained HIV-1 RNA <50 copies/mL at Week 240 (missing = excluded); when missing virologic data were considered as failure, 67.2% (95% CI [63.4%-70.8%], 426/634) maintained HIV-1 RNA <50 copies/mL. Mean (SD) change in CD4+ count from baseline was +338 (236.2) cells/μL. No treatment-emergent resistance to B/F/TAF was detected. Adverse events led to drug discontinuation in 1.6% (n = 10/634) of participants (n = 5 with events considered drug-related). No discontinuations were due to renal adverse events. Median (IQR) total cholesterol increased 21 (1,42) mg/dL from baseline; the change in total cholesterol:HDL was 0.1 (-0.5,0.6). Median (IQR) weight change from baseline was +6.1 kg (2.0, 11.7) at Week 240. In Study 1489, hip and spine bone mineral density mean percent changes from baseline were ≤0.6%.
Interpretation: Through 5 years of follow-up, B/F/TAF maintained high rates of virologic suppression with no treatment-emergent resistance and rare drug discontinuations due to adverse events. These results demonstrate the durability and safety of B/F/TAF in people with HIV.
Funding: Gilead Sciences.
Keywords: Antiretroviral therapy; Bone safety; Integrase strand transfer inhibitor; Long-term; Renal safety.
© 2023 The Authors.
Conflict of interest statement
Paul Sax has received grants or contracts support from Gilead Sciences and ViiV Healthcare; consulting fees from Gilead Sciences, ViiV Healthcare, Janssen Pharmaceuticals, and Merck; and has served on board(s) for Merck. José R. Arribas has received grants or contracts and support for travel from ViiV Healthcare and Gilead Sciences, consulting fees from ViiV Healthcare, Gilead Sciences, MSD, Janssen Pharmaceuticals, and Aelix, and speaking honoraria from ViiV Healthcare, Gilead Sciences, and MSD; Chloe Orkin has received grants or contracts from Gilead Sciences, MSD, GSK, Janssen Pharmaceuticals, ViiV Healthcare, and AstraZeneca, speaking honoraria from Gilead Sciences, MSD, GSK, Janssen Pharmaceuticals, and ViiV Healthcare, and travel support from ViiV Healthcare and has served as president of the Medical Womens Federation and a governing council member for the International AIDS Society; Adriano Lazzarin and Yazdan Yazdanpanah have declared no interests; Anton Pozniak has received grant support from Gilead Sciences, Janssen Pharmaceuticals, ViiV Healthcare, and Merck, consulting fees from ViiV Healthcare, Merck, and Gilead Sciences, speaking honoraria from Gilead Sciences, Janssen Pharmaceuticals, ViiV Healthcare, and Merck, and travel support from Gilead Sciences and has served on boards for MRC Penta Studies, BHIV A Guidelines, and EACS Guidelines. Edwin DeJesus has participated in clinical trials for Gilead Sciences, ViiV Healthcare, Merck, AbbVie, and TheraTechnologies/Taimed. Franco Maggiolo has received consulting fees from ViiV Healthcare, Gilead Sciences, MSD, and Janssen Pharmaceuticals. Hans-Jürgen Stellbrink has received grants or contracts support, consulting fees, and speaking honoraria from Gilead Sciences, ViiV Healthcare, Janssen-Cilag, and MSD Sharp & Dohme; travel support from Gilead Sciences; has served on boards for Gilead Sciences, ViiV Healthcare, and MSD Sharp & Dohme; and has received non-financial support for either equipment, materials, drugs, medical writing, gifts, or other services from Gilead Sciences. Rima Acosta, Hailin Huang, Jason T. Hindman, Hal Martin, and Jared M. Baeten are current or former employees of Gilead Sciences and hold stock in the company. David Wohl has received support for the present manuscript from Gilead Sciences, grants or contracts support from Gilead Sciences, ViiV Healthcare, and Merck; and consulting fees and speaking honoraria from Gilead Sciences, ViiV Healthcare, Janssen Pharmaceuticals, and Merck.
Figures
References
-
- Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services; 2022. https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv Available at:
-
- Gallant J., Lazzarin A., Mills A., et al. Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised controlled non-inferiority trial. Lancet. 2017;390(10107):2063–2072. - PubMed
-
- Sax P.E., Pozniak A., Montes M.L., et al. Coformulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection (GS-US-380-1490): a randomised, double-blind, multicentre, phase 3, non-inferiority trial. Lancet. 2017;390(10107):2073–2082. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
