

Evaluation of the up-to-7 criterion for determining the treatment of hepatocellular carcinoma in Barcelona Clinic Liver Cancer stage B: a single-center retrospective cohort study
- PMID: 37201043
- PMCID: PMC10186506
- DOI: 10.21037/jgo-23-69
Evaluation of the up-to-7 criterion for determining the treatment of hepatocellular carcinoma in Barcelona Clinic Liver Cancer stage B: a single-center retrospective cohort study
Abstract
Background: At present, there are still disputes on the treatment of surgery for patients with stage B hepatocellular carcinoma (HCC). This study sought to investigate whether the up-to-7 criterion could be used to decide the treatment for HCC in Barcelona Clinic Liver Cancer stage B (BCLC-B).
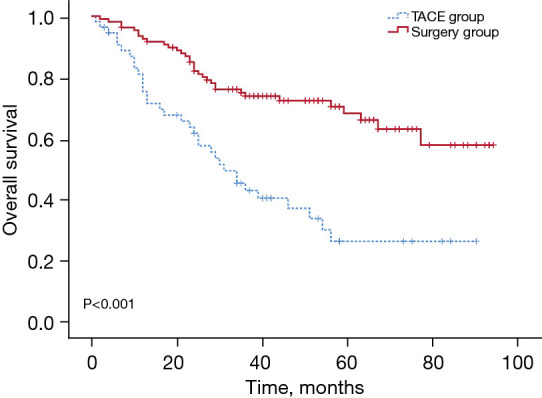
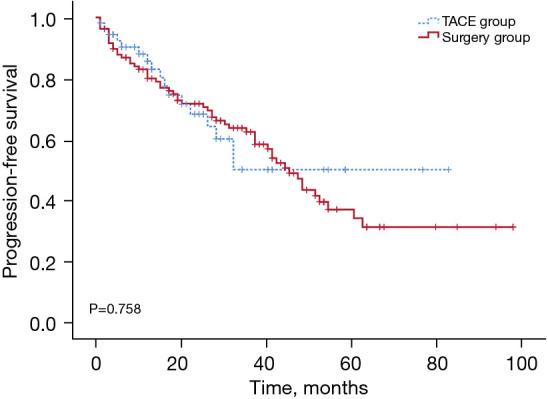
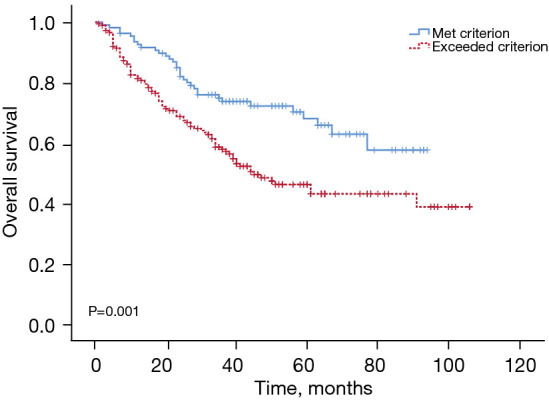
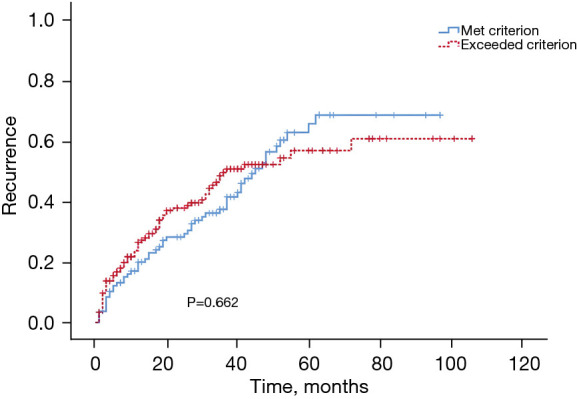
Methods: We analyzed 340 patients with HCC in BCLC-B who treated with hepatectomy or transcatheter arterial chemoembolization (TACE). Of the 285 HCC patients who underwent hepatectomy, 108 met the up-to-7 criterion and 177 exceeded it. All 55 patients in the TACE group met the up-to-7 criterion. We obtained the tumor status of the patients through inpatient medical records, outpatient medical records, and telephone follow-up of the hospital. We compared overall survival (OS) and progression-free survival (PFS) were compared between patients who met the up-to-7 criterion and who underwent either hepatectomy or TACE. OS and recurrence time were also compared between the patients who were treated with hepatectomy and who either met or exceeded the up-to-7 criterion. Across BCLC-B patients, we compared the OS of patients after surgical treatment between subgroups stratified by tumor number and diameter.
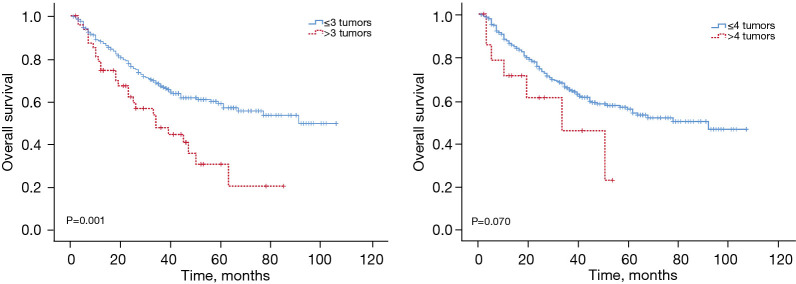
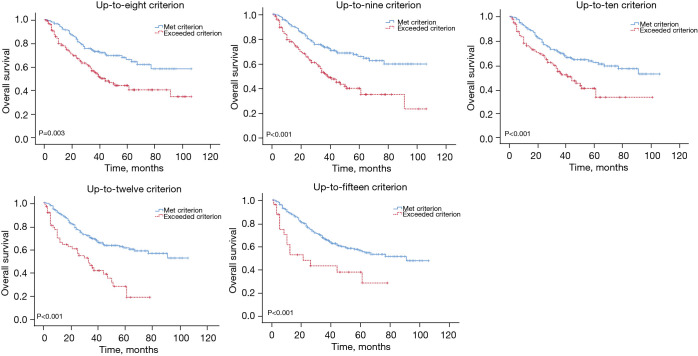
Results: Patients who met the up-to-7 criterion had significantly higher OS rates after hepatectomy than TACE (P<0.001). However, the 2 groups did not differ in terms of PFS (P=0.758). Among the patients treated by hepatectomy, the OS rates were significantly higher in patients who met the up-to-7 criterion than in those who exceeded it (P=0.001). The recurrence rates did not differ between patients who met or exceeded the criterion (P=0.662). OS was significantly higher in patients with ≤3 tumors than those with >3 tumors (P=0.001). When we stratified patients with ≤3 tumors based in whether they met or exceeded the up-to-8 to up-to-15 criterion, OS was significantly better among those who met the criterion in all cases.
Conclusions: Hepatectomy appears to be associated with better survival than TACE in patients with BCLC-B HCC who meet the up-to-7 criterion, but this criterion is not a strict indication for deciding whether to treat patients with BCLC-B surgically. Tumor number strongly affects the prognosis of BCLC-B patients after hepatectomy.
Keywords: Hepatocellular carcinoma (HCC); hepatectomy; transcatheter arterial chemoembolization (TACE); up-to-7 criterion.
2023 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-23-69/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Comparison of overall survival on surgical resection versus transarterial chemoembolization with or without radiofrequency ablation in intermediate stage hepatocellular carcinoma: a propensity score matching analysis.BMC Gastroenterol. 2020 Apr 10;20(1):99. doi: 10.1186/s12876-020-01235-w. BMC Gastroenterol. 2020. PMID: 32272898 Free PMC article.
-
Hepatectomy for ruptured hepatocellular carcinoma classified as Barcelona Clinic Liver Cancer stage 0/A: The optimal treatment.Eur J Surg Oncol. 2022 Sep;48(9):2014-2022. doi: 10.1016/j.ejso.2022.05.006. Epub 2022 May 13. Eur J Surg Oncol. 2022. PMID: 35595579
-
Improved clinical outcome using transarterial chemoembolization combined with radiofrequency ablation for patients in Barcelona clinic liver cancer stage A or B hepatocellular carcinoma regardless of tumor size: results of a single-center retrospective case control study.BMC Cancer. 2019 Oct 22;19(1):983. doi: 10.1186/s12885-019-6237-5. BMC Cancer. 2019. PMID: 31640620 Free PMC article.
-
Liver resection versus transarterial chemoembolization for the initial treatment of Barcelona Clinic Liver Cancer stage B hepatocellular carcinoma.Hepatol Int. 2018 Sep;12(5):417-428. doi: 10.1007/s12072-018-9888-4. Epub 2018 Aug 2. Hepatol Int. 2018. PMID: 30073454
-
Transarterial chemoembolization in hepatocellular carcinoma treatment: Barcelona clinic liver cancer staging system.World J Gastroenterol. 2015 Sep 28;21(36):10327-35. doi: 10.3748/wjg.v21.i36.10327. World J Gastroenterol. 2015. PMID: 26420959 Free PMC article. Review.
Cited by
-
Efficacy of therapies for intermediate-stage hepatocellular carcinoma: systematic review and network meta-analysis.Front Immunol. 2025 Jul 9;16:1577614. doi: 10.3389/fimmu.2025.1577614. eCollection 2025. Front Immunol. 2025. PMID: 40703528 Free PMC article.
-
Real-world effectiveness and safety of TACE combined with lenvatinib plus immune checkpoint inhibitors in patients with BCLC-B stage hepatocellular carcinoma.J Gastrointest Oncol. 2025 Feb 28;16(1):176-190. doi: 10.21037/jgo-2025-33. Epub 2025 Feb 26. J Gastrointest Oncol. 2025. PMID: 40115929 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous