

Advances in pre-treatment evaluation of pancreatic ductal adenocarcinoma: a narrative review
- PMID: 37201095
- PMCID: PMC10186502
- DOI: 10.21037/jgo-22-1034
Advances in pre-treatment evaluation of pancreatic ductal adenocarcinoma: a narrative review
Abstract
Background and objective: Despite advances in the multidisciplinary management of pancreatic cancer, overall prognosis remains poor, due to early progression of the disease. There is a need to also take action in staging, to make it increasingly accurate and complete, to define the setting of the therapeutic strategy. This review was planned to update the current status of pre-treatment evaluation for pancreatic cancer.
Methods: We conducted an extensive review, including relevant articles dealing with traditional imaging, functional imaging and minimally invasive surgical procedures before treatment for pancreatic cancer. We searched articles written in English only. Data in the PubMed database, published in the period between January 2000 and January 2022, were retrieved. Prospective observational studies, retrospective analyses and meta-analyses were reviewed and analysed.
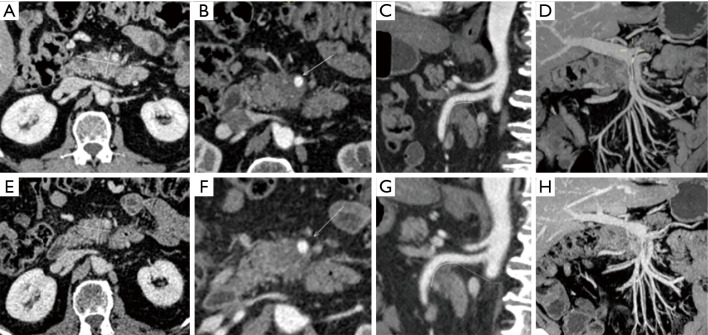
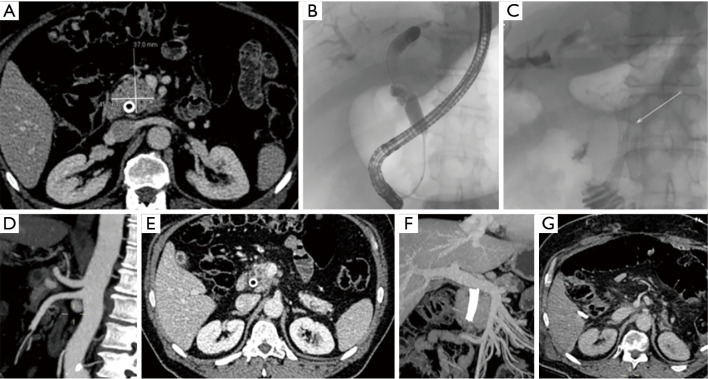
Key content and findings: Each imaging modality (endoscopic ultrasonography, endoscopic retrograde cholangiopancreatography, computed tomography, positron emission tomography/computed tomography, staging laparoscopy) has its own diagnostic advantages and limitations. The sensitivity, specificity and accuracy for each image set are reported. Data that support the increasing role of neoadjuvant therapy (radiotherapy and chemotherapy) and the meaning of a patient-tailored treatment selection, based on tumour staging, are also discussed.
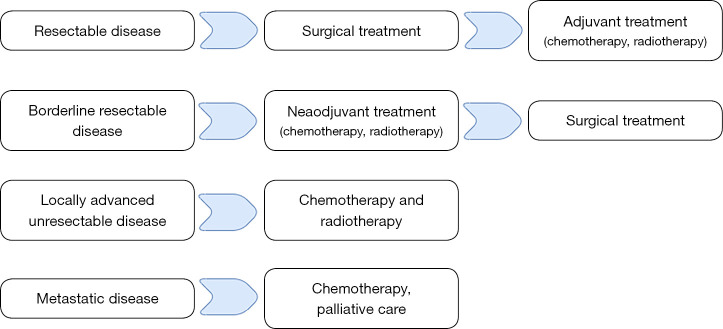
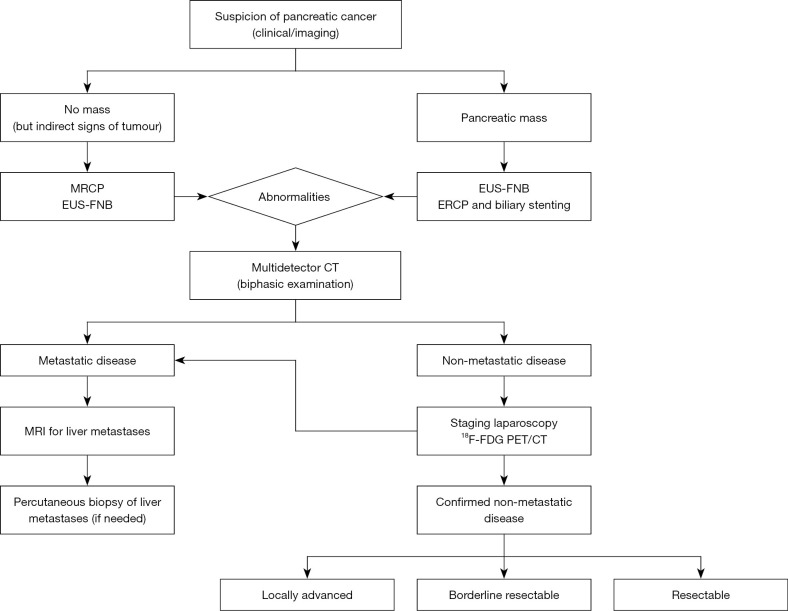
Conclusions: A multimodal pre-treatment workup should be searched as it improves staging accuracy, orienting patients with resectable tumors towards surgery, optimizing patient selection with locally advanced tumors to neoadjuvant or definite therapy and avoiding surgical resection or curative radiotherapy in those with metastatic disease.
Keywords: Pancreatic cancer; imaging; laparoscopy; staging.
2023 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-1034/coif). The series “Pancreas Surgery” was commissioned by the editorial office without any funding or sponsorship. AC served as the unpaid Guest Editor of the series. The authors have no other conflicts of interest to declare.
Figures
References
-
- National Cancer Institute. Cancer Stat Facts: Pancreatic Cancer. Surveillance, Epidemiology and End Results Program. 2019.
Publication types
LinkOut - more resources
Full Text Sources