

Antithrombin Deficiency Is Associated with Prothrombotic Plasma Fibrin Clot Phenotype
- PMID: 37201530
- PMCID: PMC10460956
- DOI: 10.1055/s-0043-1768712
Antithrombin Deficiency Is Associated with Prothrombotic Plasma Fibrin Clot Phenotype
Abstract
Background: Deficiency of antithrombin increases risk of venous thromboembolism. We hypothesized that antithrombin deficiency affects fibrin clot structure and function.
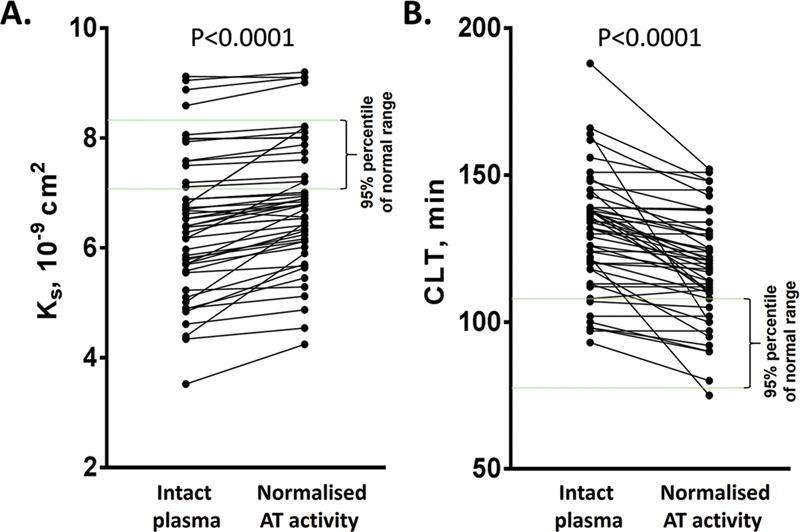
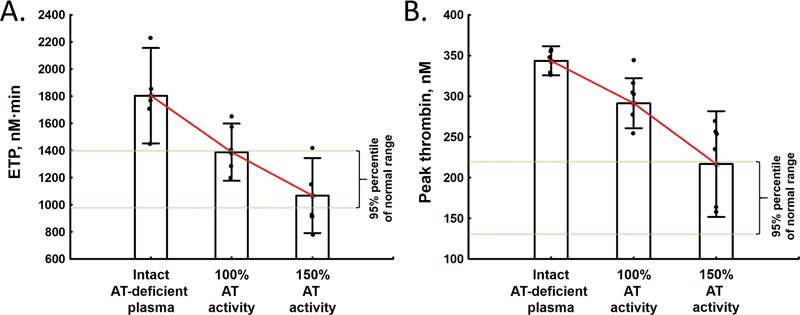
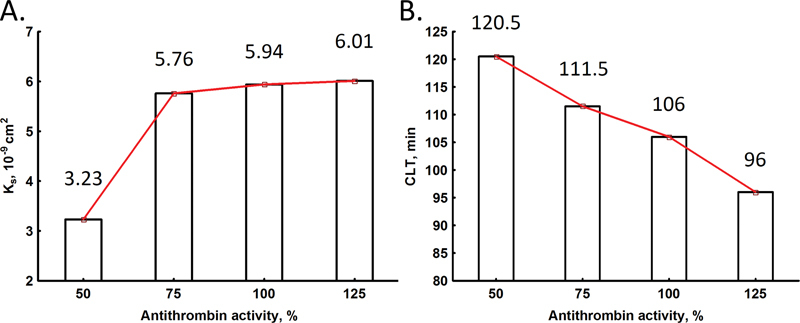
Methods: We evaluated 148 patients (age: 38 [32-50] years; 70% women) with genetically confirmed antithrombin deficiency and 50 healthy controls. Fibrin clot permeability (Ks) and clot lysis time (CLT) along with thrombin generation capacity were assessed before and after antithrombin activity normalization in vitro.
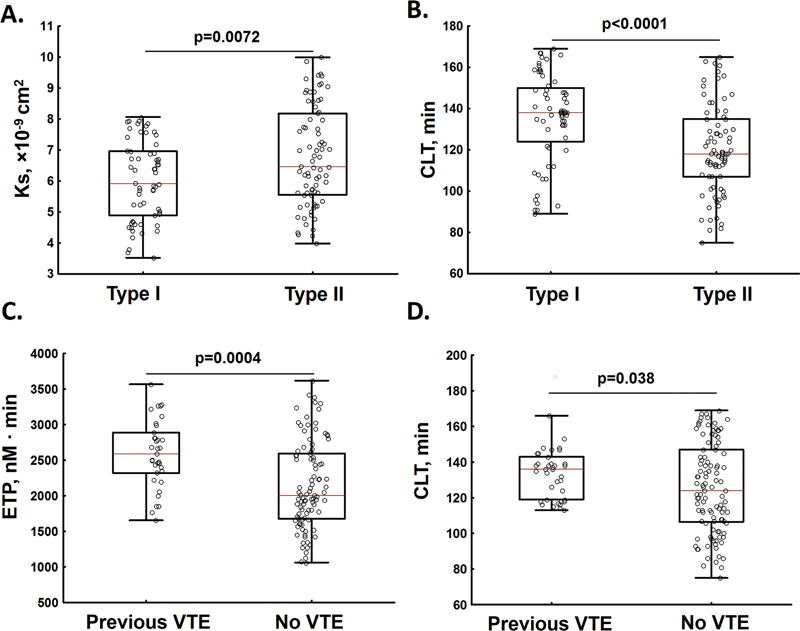
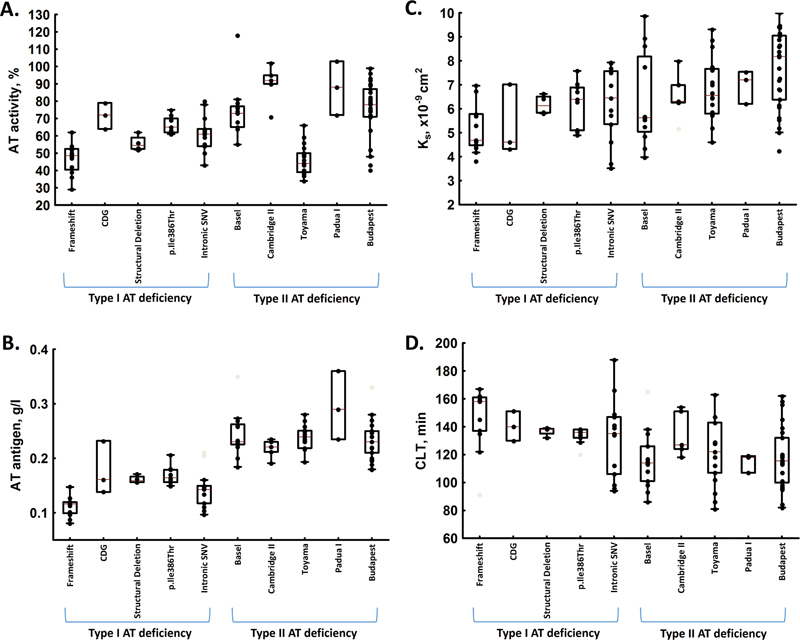
Results: Antithrombin-deficient patients had lower antithrombin activity (-39%) and antigen levels (-23%) compared with controls (both p < 0.01). Prothrombin fragment 1 + 2 levels were 26.5% higher in patients with antithrombin deficiency than in controls along with 94% increased endogenous thrombin potential (ETP) and 108% higher peak thrombin (all p < 0.01). Antithrombin deficiency was associated with 18% reduced Ks and 35% prolonged CLT (both p < 0.001). Patients with type I (n = 65; 43.9%) compared with type II antithrombin deficiency (n = 83; 56.1%) had 22.5% lower antithrombin activity (p < 0.001) and despite similar fibrinogen levels, 8.4% reduced Ks, 18% prolonged CLT, and 30% higher ETP (all p < 0.01). Reduced Ks was associated with lower antithrombin antigen level (β = - 6.1, 95% confidence interval [CI]: -1.7 to -10.5), while prolonged CLT was associated with lower antithrombin antigen (β = - 69.6, 95% CI: -9.6 to -129.7), activity (β = - 2.4, 95% CI: -0.3 to -4.5), higher PAI-1 (β = 12.1, 95% CI: 7.7-16.5), and thrombin-activatable fibrinolysis inhibitor levels (β = 3.8, 95% CI: 1.9-5.7). Addition of exogenous antithrombin reduced ETP (-42%) and peak thrombin (-21%), and improved Ks (+8%) and CLT (-12%; all p < 0.01).
Conclusion: Our study suggests that enhanced thrombin generation and prothrombotic plasma fibrin clot phenotype can contribute to increased risk of thrombosis in patients with antithrombin deficiency.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
None declared.
Figures
References
-
- Patnaik M M, Moll S. Inherited antithrombin deficiency: a review. Haemophilia. 2008;14(06):1229–1239. - PubMed
-
- Limperger V, Franke A, Kenet G et al.Clinical and laboratory characteristics of paediatric and adolescent index cases with venous thromboembolism and antithrombin deficiency. An observational multicentre cohort study. Thromb Haemost. 2014;112(03):478–485. - PubMed
-
- Croles F N, Borjas-Howard J, Nasserinejad K, Leebeek F WG, Meijer K. Risk of venous thrombosis in antithrombin deficiency: a systematic review and Bayesian meta-analysis. Semin Thromb Hemost. 2018;44(04):315–326. - PubMed
-
- For the Plasma Coagulation Inhibitors Subcommittee of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis . Lane D A, Bayston T, Olds R J et al.Antithrombin mutation database: 2nd (1997) update. Thromb Haemost. 1997;77(01):197–211. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous