

Optimized preoperative planning of double outlet right ventricle patients by 3D printing and virtual reality: a pilot study
- PMID: 37202357
- PMCID: PMC10481772
- DOI: 10.1093/icvts/ivad072
Optimized preoperative planning of double outlet right ventricle patients by 3D printing and virtual reality: a pilot study
Abstract
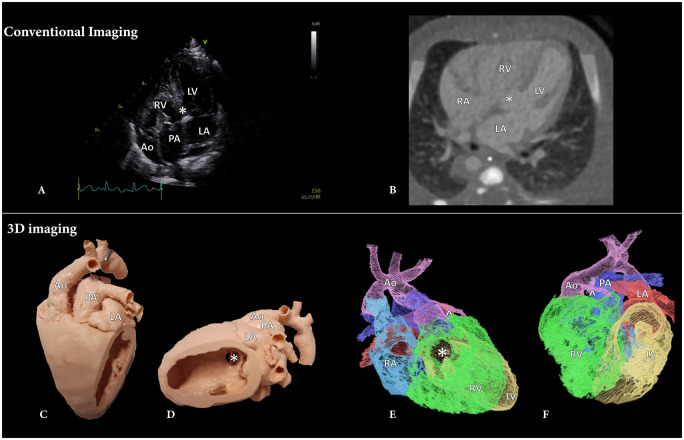
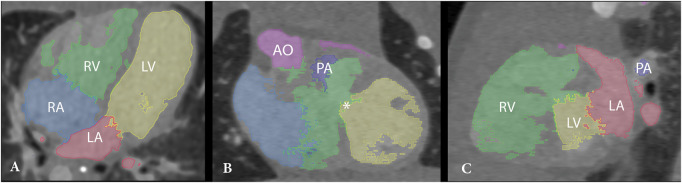
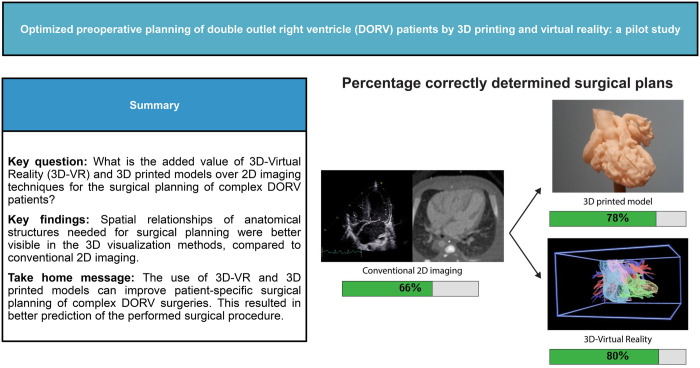
Objectives: In complex double outlet right ventricle (DORV) patients, the optimal surgical approach may be difficult to assess based on conventional 2-dimensional (2D) ultrasound (US) and computed tomography (CT) imaging. The aim of this study is to assess the added value of 3-dimensional (3D) printed and 3D virtual reality (3D-VR) models of the heart used for surgical planning in DORV patients, supplementary to the gold standard 2D imaging modalities.
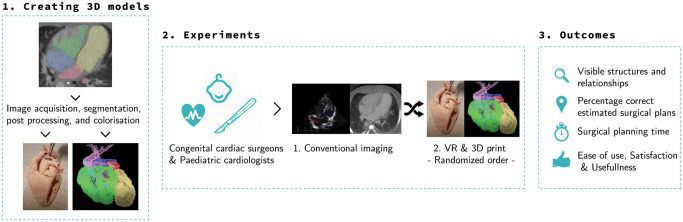
Methods: Five patients with different DORV subtypes and high-quality CT scans were selected retrospectively. 3D prints and 3D-VR models were created. Twelve congenital cardiac surgeons and paediatric cardiologists, from 3 different hospitals, were shown 2D-CT first, after which they assessed the 3D print and 3D-VR models in random order. After each imaging method, a questionnaire was filled in on the visibility of essential structures and the surgical plan.
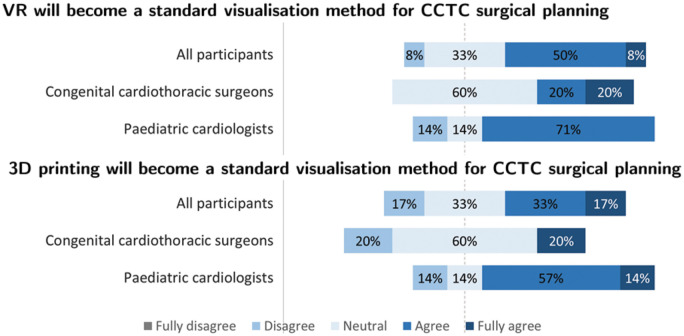
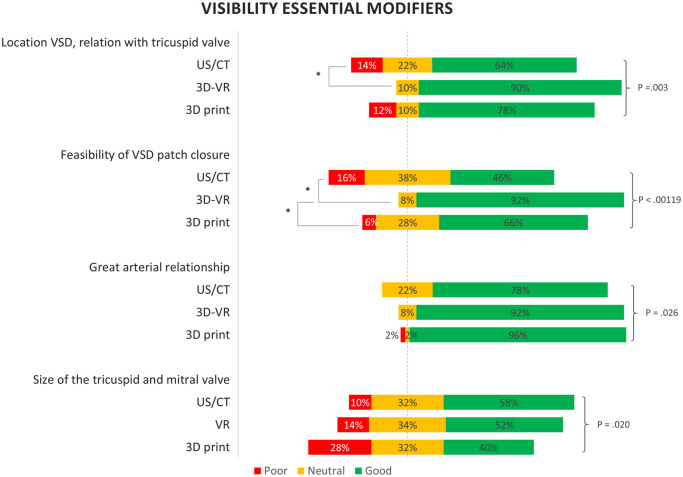
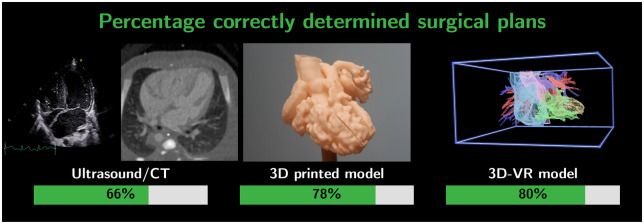
Results: Spatial relationships were generally better visualized using 3D methods (3D printing/3D-VR) than in 2D. The feasibility of ventricular septum defect patch closure could be determined best using 3D-VR reconstructions (3D-VR 92%, 3D print 66% and US/CT 46%, P < 0.01). The percentage of proposed surgical plans corresponding to the performed surgical approach was 66% for plans based on US/CT, 78% for plans based on 3D printing and 80% for plans based on 3D-VR visualization.
Conclusions: This study shows that both 3D printing and 3D-VR have additional value for cardiac surgeons and cardiologists over 2D imaging, because of better visualization of spatial relationships. As a result, the proposed surgical plans based on the 3D visualizations matched the actual performed surgery to a greater extent.
Keywords: 3D printing; Congenital cardiac surgery; Congenital heart disease; Double outlet right ventricle; Surgical planning; Virtual reality.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Similar articles
-
Enhanced 3D visualization for planning biventricular repair of double outlet right ventricle: a pilot study on the advantages of virtual reality.Eur Heart J Digit Health. 2021 Oct 28;2(4):667-675. doi: 10.1093/ehjdh/ztab087. eCollection 2021 Dec. Eur Heart J Digit Health. 2021. PMID: 36713107 Free PMC article.
-
Three-dimensional printing and virtual reconstruction in surgical planning of double-outlet right ventricle repair.JTCVS Tech. 2022 Nov 26;17:138-150. doi: 10.1016/j.xjtc.2022.11.005. eCollection 2023 Feb. JTCVS Tech. 2022. PMID: 36820361 Free PMC article.
-
Clinical Application and Multidisciplinary Assessment of Three Dimensional Printing in Double Outlet Right Ventricle With Remote Ventricular Septal Defect.World J Pediatr Congenit Heart Surg. 2016 May;7(3):344-50. doi: 10.1177/2150135116645604. World J Pediatr Congenit Heart Surg. 2016. PMID: 27142402
-
3D Printing in Surgical Management of Double Outlet Right Ventricle.Front Pediatr. 2018 Jan 10;5:289. doi: 10.3389/fped.2017.00289. eCollection 2017. Front Pediatr. 2018. PMID: 29379778 Free PMC article. Review.
-
Role of virtual reality in congenital heart disease.Congenit Heart Dis. 2018 May;13(3):357-361. doi: 10.1111/chd.12587. Epub 2018 Feb 5. Congenit Heart Dis. 2018. PMID: 29399969 Review.
Cited by
-
Using Multimodality Imaging and 3-Dimensional Printed Models to Guide Decision-Making for Complex Congenital Biventricular Repair.JACC Case Rep. 2025 Jun 25;30(16):103884. doi: 10.1016/j.jaccas.2025.103884. JACC Case Rep. 2025. PMID: 40579094 Free PMC article.
-
Digital Transformation in Thoracic Surgery: a survey among the European Society of Thoracic Surgeons.Interdiscip Cardiovasc Thorac Surg. 2024 Jul 3;39(1):ivae119. doi: 10.1093/icvts/ivae119. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 38941504 Free PMC article.
-
Unifocalization of Major Aortopulmonary Collateral Arteries (MAPCAs) and Native Pulmonary Arteries in Infancy-Application of 3D Printing and Virtual Reality.J Cardiovasc Dev Dis. 2024 Dec 13;11(12):403. doi: 10.3390/jcdd11120403. J Cardiovasc Dev Dis. 2024. PMID: 39728293 Free PMC article.
References
-
- Peixoto LB, Leal SMB, Silva CES, Moreira SML, Ortiz J.. Double outlet right ventricle with anterior and left-sided aorta and subpulmonary ventricular septal defect. Arq Bras Cardiol 1999;73:446–50. - PubMed
-
- Yim D, Dragulescu A, Ide H, Seed M, Grosse-Wortmann L, Van Arsdell G. et al. Essential modifiers of double outlet right ventricle: revisit with endocardial surface images and 3-dimensional print models. Circ Cardiovasc Imaging 2018;11:e006891. - PubMed
-
- Valverde I, Gomez G, Gonzalez A, Suarez-Mejias C, Adsuar A, Coserria JF. et al. Three-dimensional patient-specific cardiac model for surgical planning in Nikaidoh procedure. Cardiol Young 2015;25:698–704. - PubMed
-
- Cen J, Liufu R, Wen S, Qiu H, Liu X, Chen X. et al. Three-dimensional printing, virtual reality and mixed reality for pulmonary atresia: early surgical outcomes evaluation. Hear Lung Circ 2021;30:296–302. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
