

Abdominal visceral tuberculosis: a malignancy mimic
- PMID: 37204509
- PMCID: PMC10197054
- DOI: 10.1007/s00261-023-03939-5
Abdominal visceral tuberculosis: a malignancy mimic
Abstract
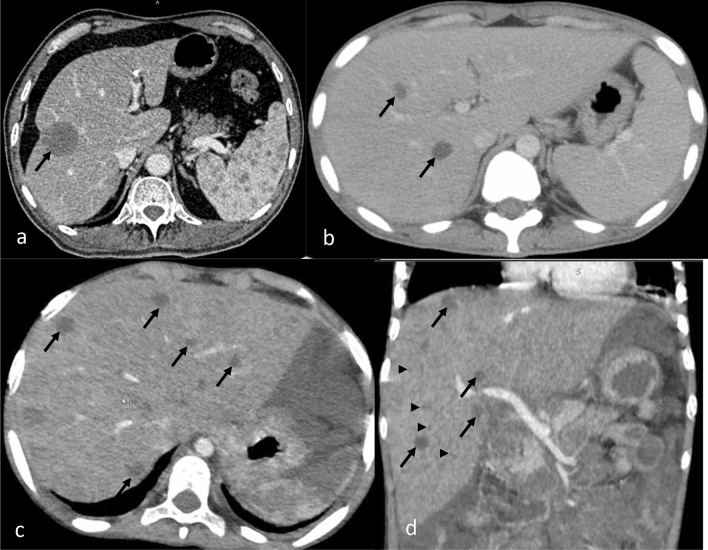
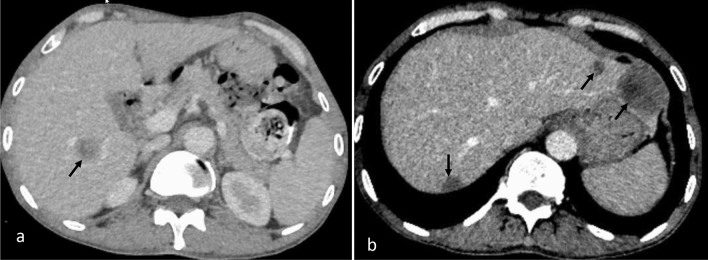
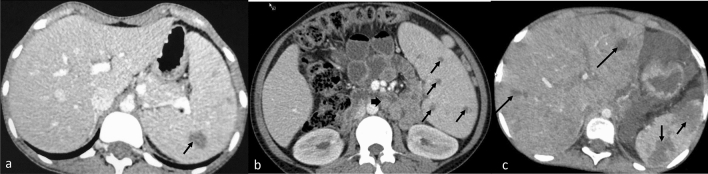
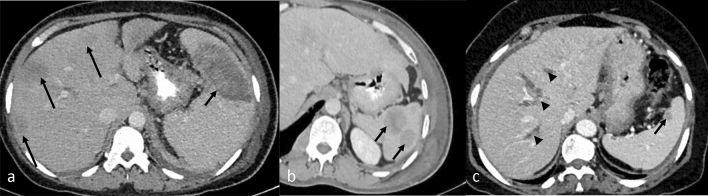
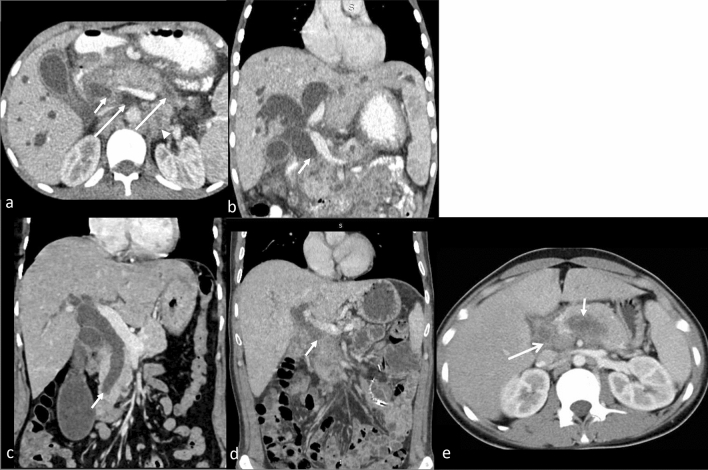
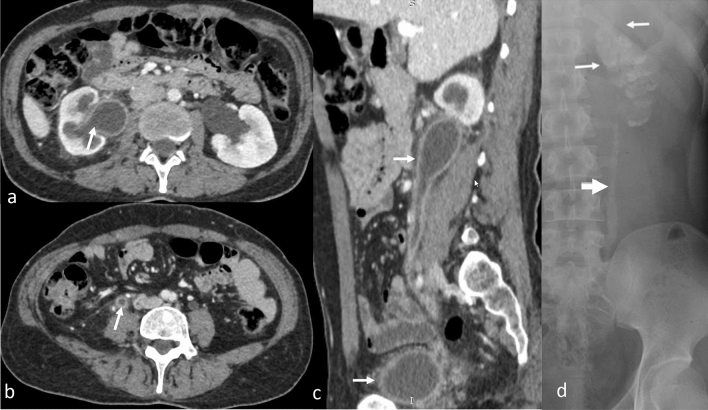
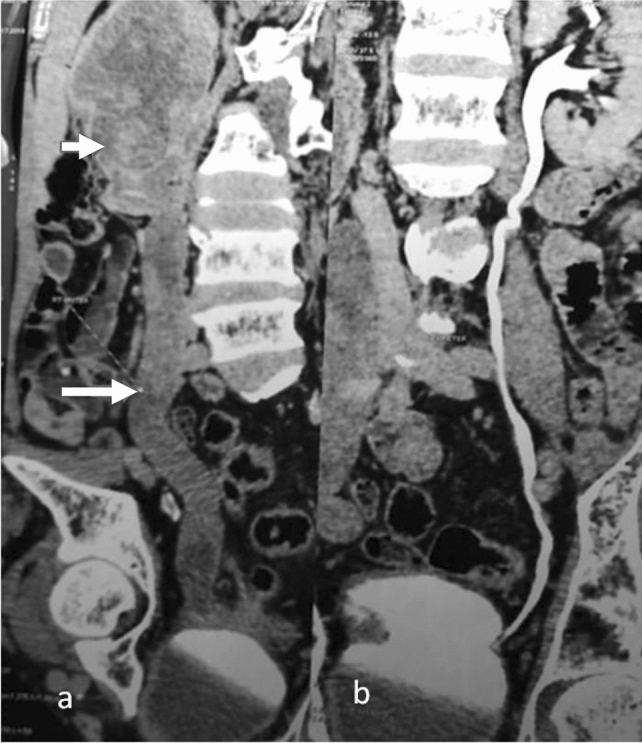
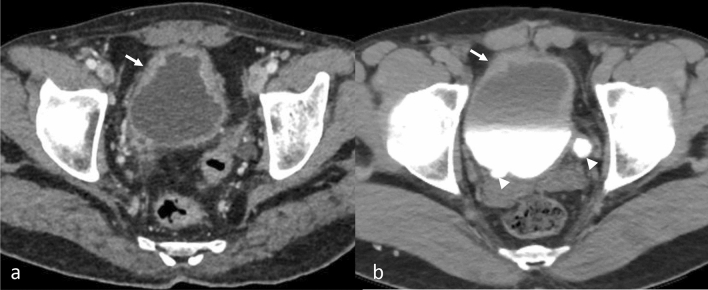
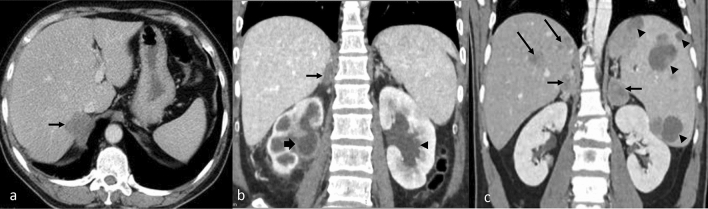
The purpose is to discuss abdominal tuberculosis mimicking malignancy involving the abdominal viscera. TB of the abdominal viscera is common, especially in countries where tuberculosis is endemic and in pockets of non-endemic countries. Diagnosis is challenging as clinical presentations are often non-specific. Tissue sampling may be necessary for definitive diagnosis. Awareness of the early and late disease imaging appearances of abdominal tuberculosis involving the viscera that can mimic malignancy can aid detecting TB, providing a differential diagnosis, assessing extent of spread, guiding biopsy, and evaluating response.
Keywords: Abdominal viscera; CT; Cancer; MRI; Tuberculosis; Ultrasonography.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors have no competing interests to declare that are relevant to the content of this article.
Figures
References
-
- Trends in Tuberculosis, 2021 [Internet]. Centers for Disease Control and Prevention; [cited 2023 Apr 18]. Available from: https://www.cdc.gov/tb/publications/factsheets/statistics/tbtrends.htm
-
- Padma V, Anand NN, Rajendran SM, Gurukal S. Primary tuberculosis of stomach. J Indian Med Assoc. 2012;110(3):187–188. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
