

A porcine study of ultrasound-guided versus fluoroscopy-guided placement of endovascular balloons in the inferior vena cava (REBOVC) and the aorta (REBOA)
- PMID: 37205275
- PMCID: PMC10186488
- DOI: 10.1136/tsaco-2022-001075
A porcine study of ultrasound-guided versus fluoroscopy-guided placement of endovascular balloons in the inferior vena cava (REBOVC) and the aorta (REBOA)
Abstract
Objectives: In fluoroscopy-free settings, alternative safe and quick methods for placing resuscitative endovascular balloon occlusion of the aorta (REBOA) and resuscitative endovascular balloon occlusion of the inferior vena cava (REBOVC) are needed. Ultrasound is being increasingly used to guide the placement of REBOA in the absence of fluoroscopy. Our hypothesis was that ultrasound could be used to adequately visualize the suprahepatic vena cava and guide REBOVC positioning, without significant time-delay, when compared with fluoroscopic guidance, and compared with the corresponding REBOA placement.
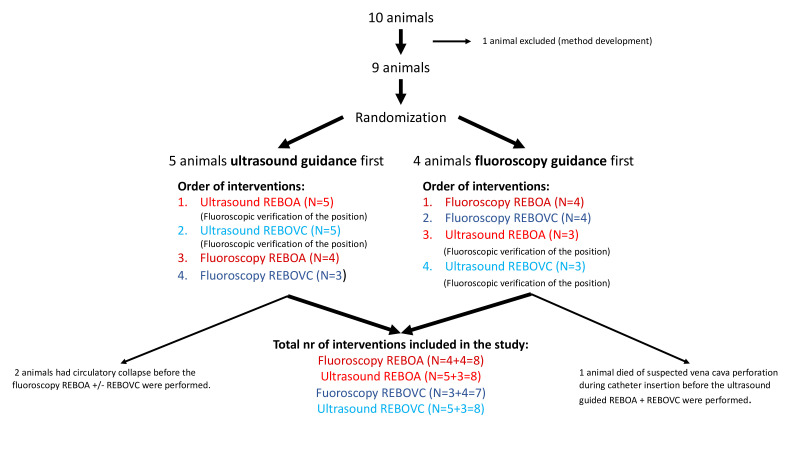
Methods: Nine anesthetized pigs were used to compare ultrasound-guided placement of supraceliac REBOA and suprahepatic REBOVC with corresponding fluoroscopic guidance, in terms of correct placement and speed. Accuracy was controlled by fluoroscopy. Four intervention groups: (1) fluoroscopy REBOA, (2) fluoroscopy REBOVC, (3) ultrasound REBOA and (4) ultrasound REBOVC. The aim was to carry out the four interventions in all animals. Randomization was performed to either fluoroscopic or ultrasound guidance being used first. The time required to position the balloons in the supraceliac aorta or in the suprahepatic inferior vena cava was recorded and compared between the four intervention groups.
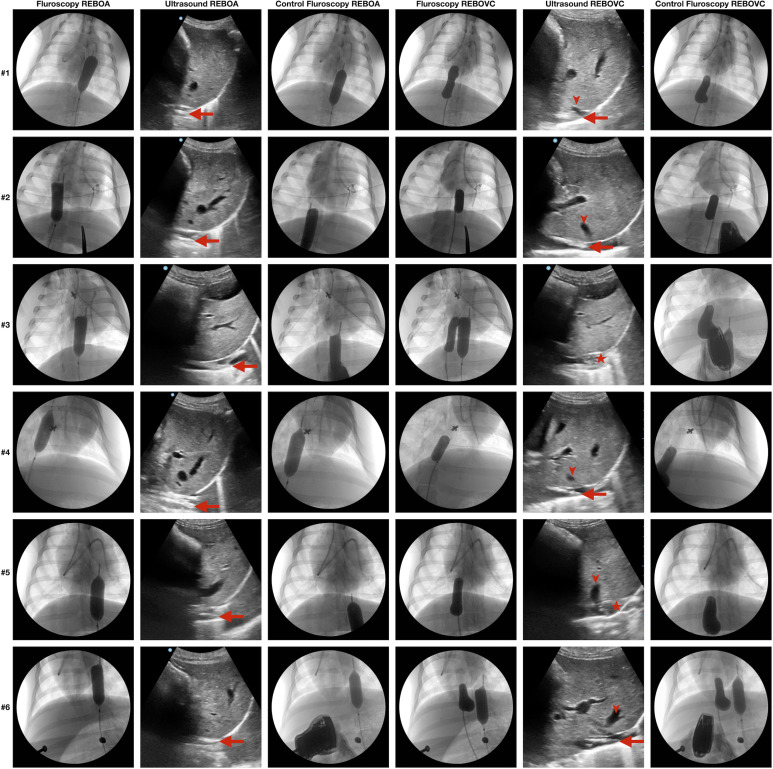
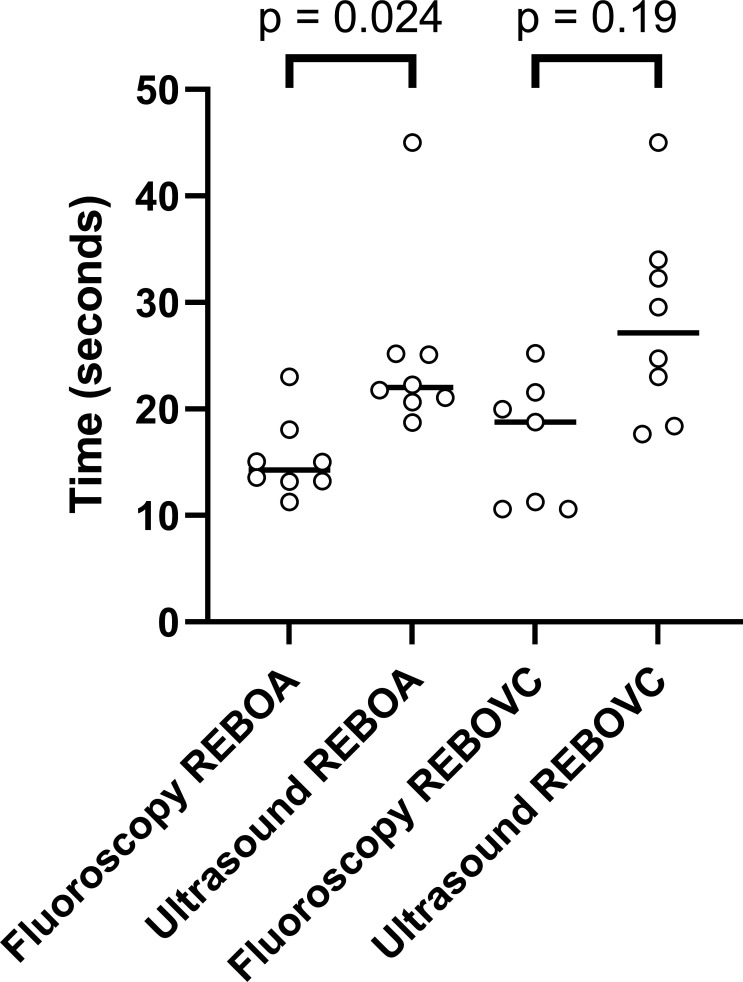
Results: Ultrasound-guided REBOA and REBOVC placement was completed in eight animals, respectively. All eight had correctly positioned REBOA and REBOVC on fluoroscopic verification. Fluoroscopy-guided REBOA placement was slightly faster (median 14 s, IQR 13-17 s) than ultrasound-guided REBOA (median 22 s, IQR 21-25 s, p=0.024). The corresponding comparisons of the REBOVC groups were not statistically significant, with fluoroscopy-guided REBOVC taking 19 s, median (IQR 11-22 s) and ultrasound-guided REBOVC taking 28 s, median (IQR 20-34 s, p=0.19).
Conclusion: Ultrasound adequately and quickly guide the placement of supraceliac REBOA and suprahepatic REBOVC in a porcine laboratory model, however, safety issues must be considered before use in trauma patients.
Level of evidence: Prospective, experimental, animal study. Basic science study.
Keywords: multiple trauma; shock, hemorrhagic; ultrasonography; veins.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JÅ has an ongoing collaboration with GE Healthcare regarding workshops in peripheral nerve blocks, but has not received any private payments. The other authors declare no conflicts of interest of the subject matter.
Figures
Similar articles
-
The effect of an endovascular Heaney maneuver to achieve total hepatic isolation on survival, hemodynamic stability, retrohepatic bleeding, and collateral flow in a porcine model.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1547-1557. doi: 10.1007/s00068-024-02482-2. Epub 2024 Mar 8. Eur J Trauma Emerg Surg. 2024. PMID: 38456908 Free PMC article.
-
A randomized porcine study of the hemodynamic and metabolic effects of combined endovascular occlusion of the vena cava and the aorta in normovolemia and in hemorrhagic shock.J Trauma Acute Care Surg. 2021 May 1;90(5):817-826. doi: 10.1097/TA.0000000000003098. J Trauma Acute Care Surg. 2021. PMID: 33496552 Free PMC article.
-
Resuscitative endovascular balloon occlusion of the inferior vena cava is made hemodynamically possible by concomitant endovascular balloon occlusion of the aorta-A porcine study.J Trauma Acute Care Surg. 2020 Jan;88(1):160-168. doi: 10.1097/TA.0000000000002467. J Trauma Acute Care Surg. 2020. PMID: 31397743
-
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) Use in Animal Trauma Models.J Surg Res. 2021 Dec;268:125-135. doi: 10.1016/j.jss.2021.06.052. Epub 2021 Jul 23. J Surg Res. 2021. PMID: 34304008 Review.
-
The resuscitative endovascular balloon occlusion of aorta (REBOA) device-what radiologists need to know.Emerg Radiol. 2019 Dec;26(6):691-694. doi: 10.1007/s10140-019-01724-w. Epub 2019 Sep 12. Emerg Radiol. 2019. PMID: 31515654 Review.
Cited by
-
The effect of an endovascular Heaney maneuver to achieve total hepatic isolation on survival, hemodynamic stability, retrohepatic bleeding, and collateral flow in a porcine model.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1547-1557. doi: 10.1007/s00068-024-02482-2. Epub 2024 Mar 8. Eur J Trauma Emerg Surg. 2024. PMID: 38456908 Free PMC article.
References
-
- Brenner M, Inaba K, Aiolfi A, DuBose J, Fabian T, Bee T, Holcomb JB, Moore L, Skarupa D, Scalea TM, et al. . Resuscitative endovascular balloon occlusion of the aorta and resuscitative thoracotomy in select patients with hemorrhagic shock: early results from the American association for the surgery of trauma’s aortic occlusion in resuscitation for trauma and acute care surgery registry. J Am Coll Surg 2018;226:730–40.:S1072-7515(18)30098-X. 10.1016/j.jamcollsurg.2018.01.044 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials