

A randomized, open-label study of the tolerability and efficacy of one or three daily doses of ivermectin plus diethylcarbamazine and albendazole (IDA) versus one dose of ivermectin plus albendazole (IA) for treatment of onchocerciasis
- PMID: 37205721
- PMCID: PMC10234528
- DOI: 10.1371/journal.pntd.0011365
A randomized, open-label study of the tolerability and efficacy of one or three daily doses of ivermectin plus diethylcarbamazine and albendazole (IDA) versus one dose of ivermectin plus albendazole (IA) for treatment of onchocerciasis
Abstract
Background: Onchocerciasis ("river blindness") has been targeted for elimination. New treatments that kill or permanently sterilize female worms could accelerate this process. Prior studies have shown that triple drug treatment with ivermectin plus diethylcarbamazine and albendazole (IDA) leads to prolonged clearance of microfilaremia in persons with lymphatic filariasis. We now report results from a randomized clinical trial that compared the tolerability and efficacy of IDA vs. a comparator treatment (ivermectin plus albendazole, IA) in persons with onchocerciasis.
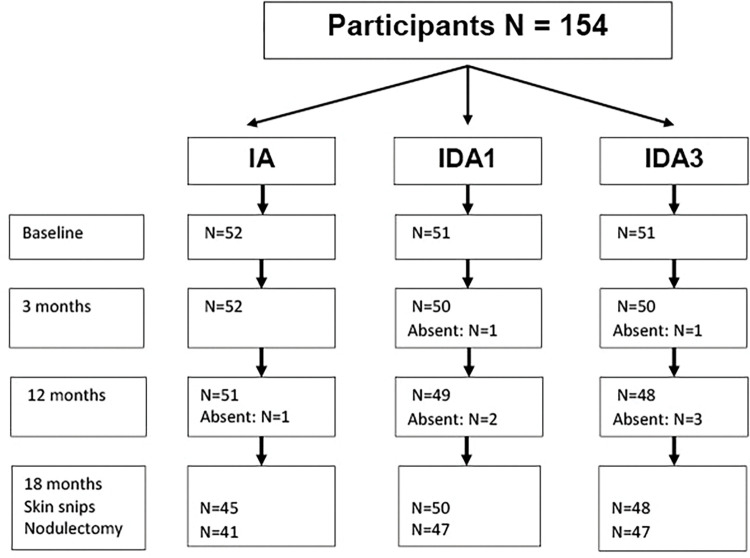
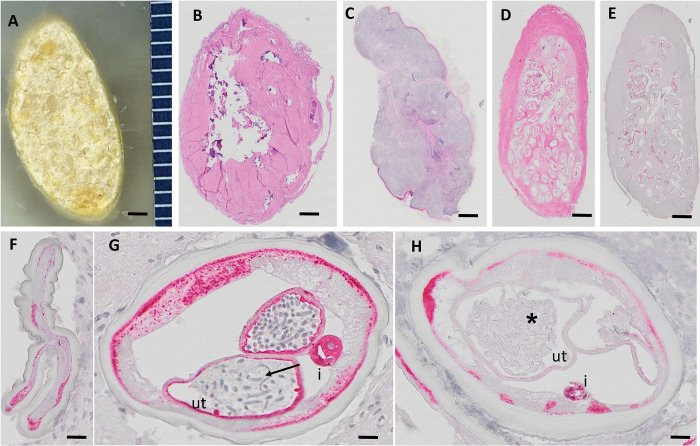
Methods and findings: The study was performed in the Volta region of Ghana. Persons with microfiladermia and palpable subcutaneous nodules were pre-treated with two oral doses of ivermectin (150 μg/kg) separated by at least 6 months prior to treatment with either a single oral dose of ivermectin 150 μg/kg plus albendazole 400 mg (IA), a single oral dose of IDA (IDA1, IA plus diethylcarbamazine (DEC. 6 mg/kg) or three consecutive daily doses of IDA (IDA3). These treatments were tolerated equally well. While adverse events were common (approximately 30% overall), no severe or serious treatment-emergent adverse events were observed. Skin microfilariae were absent or present with very low densities after all three treatments through 18 months, at which time nodules were excised for histological assessment. Nodule histology was evaluated by two independent assessors who were masked regarding participant infection status or treatment assignment. Significantly lower percentages of female worms were alive and fertile in nodules recovered from study participants after IDA1 (40/261, 15.3%) and IDA3 (34/281, 12.1%) than after IA (41/180, 22.8%). This corresponds to a 40% reduction in the percentage of female worms that were alive and fertile after IDA treatments relative to results observed after the IA comparator treatment (P = 0.004). Percentages of female worms that were alive (a secondary outcome of the study) were also lower after IDA treatments (301/574, 52.4%) than after IA (127/198, 64.1%) (P = 0.004). Importantly, some comparisons (including the reduced % of fertile female worms after IDA1 vs IA treatment, which was the primary endpoint for the study) were not statistically significant when results were adjusted for intraclass correlation of worm fertility and viability for worms recovered from individual study participants.
Conclusions: Results from this pilot study suggest that IDA was well tolerated after ivermectin pretreatment. They also suggest that IDA was more effective than the comparator treatment IA for killing or sterilizing female O. volvulus worms. No other short-course oral treatment for onchocerciasis has been demonstrated to have macrofilaricidal activity. However, this first study was too small to provide conclusive results. Therefore, additional studies will be needed to confirm these promising findings.
Trial registration: The study is registered at Cinicaltrials.gov under the number NCT04188301.
Copyright: © 2023 Opoku et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
An open label, randomized clinical trial to compare the tolerability and efficacy of ivermectin plus diethylcarbamazine and albendazole vs. diethylcarbamazine plus albendazole for treatment of brugian filariasis in Indonesia.PLoS Negl Trop Dis. 2021 Mar 29;15(3):e0009294. doi: 10.1371/journal.pntd.0009294. eCollection 2021 Mar. PLoS Negl Trop Dis. 2021. PMID: 33780481 Free PMC article. Clinical Trial.
-
Efficacy and Safety of a Single Dose of Ivermectin, Diethylcarbamazine, and Albendazole for Treatment of Lymphatic Filariasis in Côte d'Ivoire: An Open-label Randomized Controlled Trial.Clin Infect Dis. 2020 Oct 23;71(7):e68-e75. doi: 10.1093/cid/ciz1050. Clin Infect Dis. 2020. PMID: 31641754 Free PMC article. Clinical Trial.
-
An open label, block randomized, community study of the safety and efficacy of co-administered ivermectin, diethylcarbamazine plus albendazole vs. diethylcarbamazine plus albendazole for lymphatic filariasis in India.PLoS Negl Trop Dis. 2021 Feb 16;15(2):e0009069. doi: 10.1371/journal.pntd.0009069. eCollection 2021 Feb. PLoS Negl Trop Dis. 2021. PMID: 33591979 Free PMC article. Clinical Trial.
-
Antifilarial treatment strategies: a systematic review and network meta-analysis.BMC Infect Dis. 2025 May 16;25(1):712. doi: 10.1186/s12879-025-11105-z. BMC Infect Dis. 2025. PMID: 40380307 Free PMC article. Review.
-
Model-based analysis of trial data: microfilaria and worm-productivity loss after diethylcarbamazine-albendazole or ivermectin-albendazole combination therapy against Wuchereria bancrofti.Trop Med Int Health. 2006 May;11(5):718-28. doi: 10.1111/j.1365-3156.2006.01606.x. Trop Med Int Health. 2006. PMID: 16640625 Review.
Cited by
-
In Vitro Filaricidal Properties of Aqueous Extracts of Combretum nigricans (Combretaceae) on Onchocerca ochengi (Onchocercidae).J Parasitol Res. 2024 Jan 31;2024:2119056. doi: 10.1155/2024/2119056. eCollection 2024. J Parasitol Res. 2024. PMID: 38328477 Free PMC article.
-
Spatial proteomics of Onchocerca volvulus with pleomorphic neoplasms shows local and systemic dysregulation of protein expression.PLoS Negl Trop Dis. 2025 Mar 31;19(3):e0012929. doi: 10.1371/journal.pntd.0012929. eCollection 2025 Mar. PLoS Negl Trop Dis. 2025. PMID: 40163807 Free PMC article.
-
Onchocerca volvulus microfilariae in the anterior chambers of the eye and ocular adverse events after a single dose of 8 mg moxidectin or 150 µg/kg ivermectin: results of a randomized double-blind Phase 3 trial in the Democratic Republic of the Congo, Ghana and Liberia.Parasit Vectors. 2024 Mar 15;17(1):137. doi: 10.1186/s13071-023-06087-3. Parasit Vectors. 2024. PMID: 38491528 Free PMC article. Clinical Trial.
-
Genetic structuring and estimation of reproductive adults in Onchocerca volvulus: A genome-wide analysis across hosts and regions.PLoS Negl Trop Dis. 2025 Jul 1;19(7):e0013221. doi: 10.1371/journal.pntd.0013221. eCollection 2025 Jul. PLoS Negl Trop Dis. 2025. PMID: 40591654 Free PMC article.
-
Spatial proteomics of Onchocerca volvulus with pleomorphic neoplasms shows local and systemic dysregulation of protein expression.bioRxiv [Preprint]. 2024 Oct 17:2024.10.15.618383. doi: 10.1101/2024.10.15.618383. bioRxiv. 2024. Update in: PLoS Negl Trop Dis. 2025 Mar 31;19(3):e0012929. doi: 10.1371/journal.pntd.0012929. PMID: 39463952 Free PMC article. Updated. Preprint.
References
-
- WHO. Progress report on the elimination of human onchocerciasis, 2019–2020. Wkly Epidemiol Rec. 2020;95:545–56. Epub 2020/11/14. . - PubMed
-
- WHO. Progress in eliminating onchocerciasis in the WHO Region of the Americas: doxycycline treatment as an end-game strategy. Wkly Epidemiol Rec. 2019;93(47):414–9. Epub 2019/09/14.
-
- Traore MO, Sarr MD, Badji A, Bissan Y, Diawara L, Doumbia K, et al.. Proof-of-principle of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: final results of a study in Mali and Senegal. PLoS Negl Trop Dis. 2012;6(9):e1825. doi: 10.1371/journal.pntd.0001825 ; PubMed Central PMCID: PMC3441490. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
