

Low risk of new dysplastic lesions in an inflammatory bowel disease population study with dye chromoendoscopy
- PMID: 37206695
- PMCID: PMC10191734
- DOI: 10.1055/a-2048-2279
Low risk of new dysplastic lesions in an inflammatory bowel disease population study with dye chromoendoscopy
Abstract
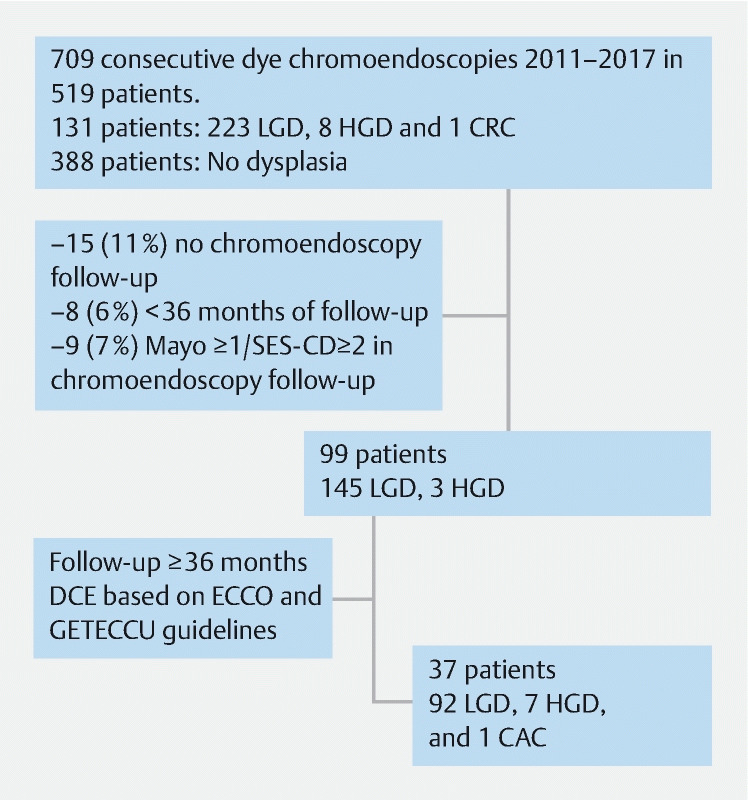
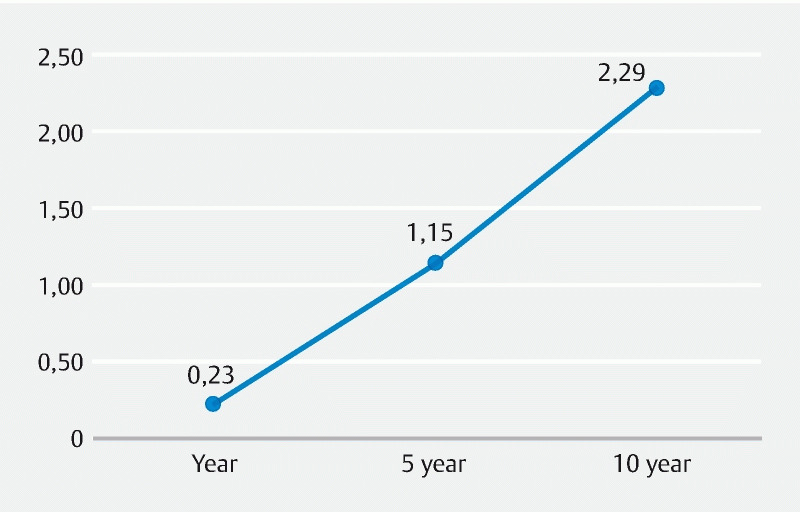
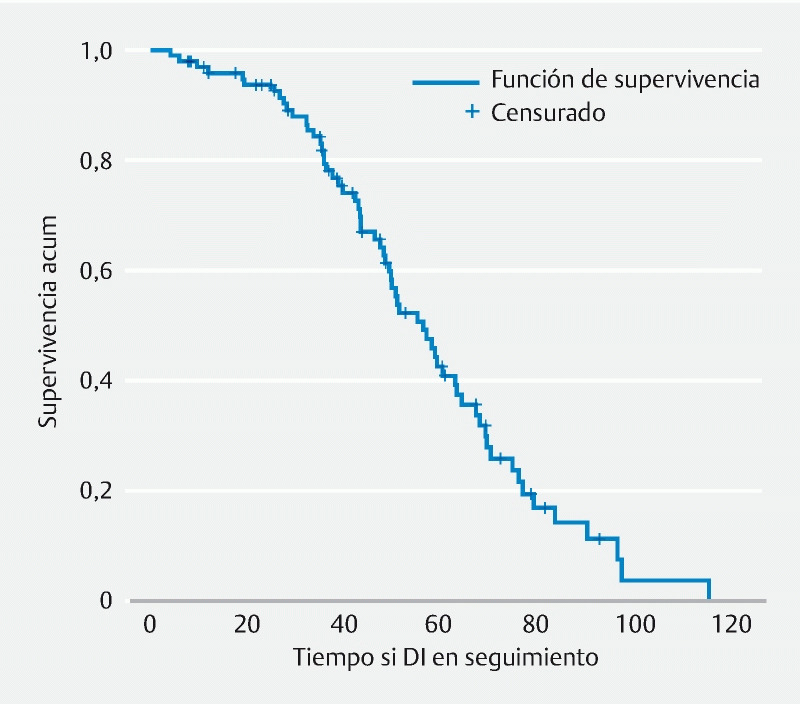
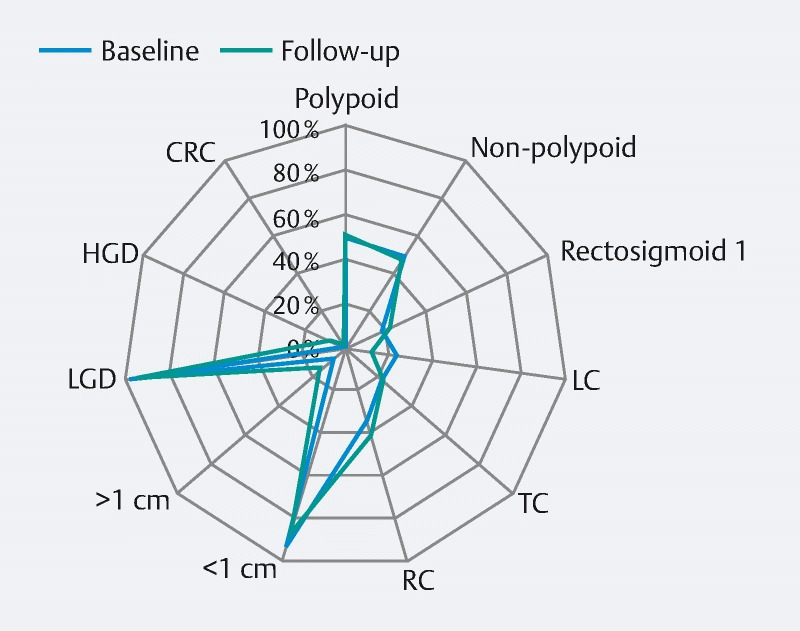
Background and study aims Rates of new dysplastic lesions or cancer progression after first dye chromoendoscopy in the era of high-definition endoscopy have yet to be determined. Patients and methods A multicenter, population-based, retrospective cohort study was performed in seven hospitals in Spain. Patients with inflammatory bowel disease and fully resected (R0) dysplastic colon lesions under surveillance with high-definition dye-based chromoendoscopy were sequentially enrolled between February 2011 and June 2017, with a minimum endoscopic follow-up of 36 months. The aim was to assess the incidence of developing more advanced metachronous neoplasia by analyzing possible associated risk factors. Results The study sample included 99 patients and 148 index lesions (145 low-grade dysplasia lesions and three high-grade dysplasia [HGD] lesions with a mean follow-up of 48.76 months [IQR: 36.34-67.15]). The overall incidence of new dysplastic lesions was 0.23 per 100 patient-years, 1.15 per 100 patients at 5 years and 2.29 per 100 patients at 10 years. A history of dysplasia was associated with a higher risk of developing any grade of dysplasia during follow-up ( P = 0.025), whereas left colon lesions were associated with a lower risk ( P = 0.043). The incidence of more advanced lesions at 1 year and 10 years was 1 % and 14 % respectively, with lesion size > 1 cm being a risk factor ( P = 0.041). One of the eight patients (13 %) with HGD lesions developed colorectal cancer during follow-up. Conclusions The risk of dysplasia progressing to advanced neoplasia and, specifically, the risk of new neoplastic lesions after endoscopic resection of colitis-associated dysplasia, are both very low.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests Dra. B. Sicilia has received support for conference attendance, speaker fees, research support and consulting fees of Abbvie, FAES, Chiesi, Dr. Falk, MSD, Tillots Pharma, Khern Pharma, Janssen, Pfizer y Takeda.
Figures
References
-
- Castaño-Mila C, Chaparro M, Gisbert J. Systematic review and meta-analysis: the declining risk of colorectal cancer in ulcerative colitis. Aliment Pharmacol Ther. 2014;39:645–659. - PubMed
-
- Imperatore M, Castiglione F, Testa A et al.Augmented endoscopy for surveillance of colonic inflammatory bowel disease: systematic review with network meta-analysis. J Crohns Colitis. 2019;13:714–724. - PubMed
-
- for the European Crohn’s and Colitis Organization [ECCO] . Magro F, Gionchetti P, Eliakim R. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J Crohns Colitis. 2017;11:649–670. - PubMed
-
- Rubin D T, Ananthakrishnan A N, Siegel C A et al.ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114:384–413. - PubMed
LinkOut - more resources
Full Text Sources