

Survival and Symptomatic Relief After Cytoreductive Hepatectomy for Neuroendocrine Tumor Liver Metastases: Long-Term Follow-up Evaluation of More Than 500 Patients
- PMID: 37208566
- PMCID: PMC10319657
- DOI: 10.1245/s10434-023-13372-z
Survival and Symptomatic Relief After Cytoreductive Hepatectomy for Neuroendocrine Tumor Liver Metastases: Long-Term Follow-up Evaluation of More Than 500 Patients
Abstract
Background: Distant metastases are the strongest predictor of poor prognosis for patients with neuroendocrine tumors (NETs). Cytoreductive hepatectomy (CRH) can relieve symptoms of hormonal excess and prolong survival for patients with liver metastases (NETLMs), but long-term outcomes are poorly characterized.
Methods: This retrospective single-institution analysis analyzed patients who underwent CRH for well-differentiated NETLMs from 2000 to 2020. Kaplan-Meier analysis estimated symptom-free interval and overall and progression-free survival. Multivariable Cox regression analysis evaluated factors associated with survival.
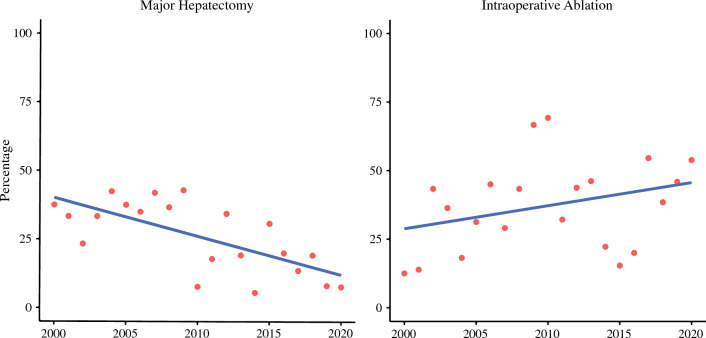
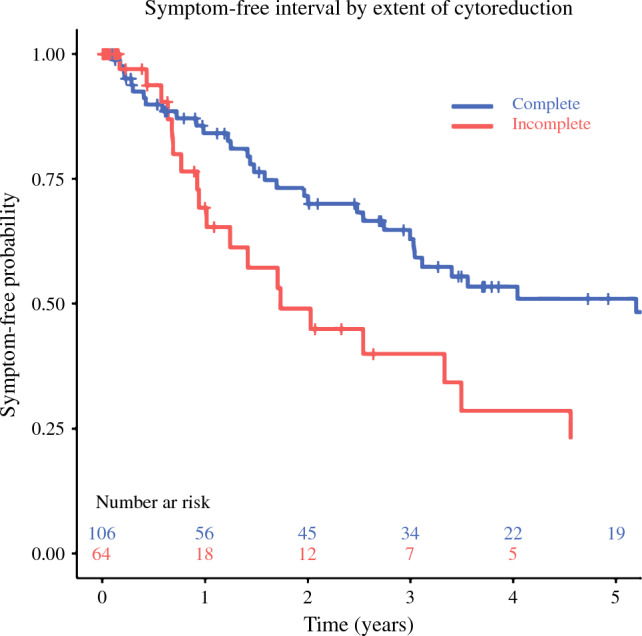
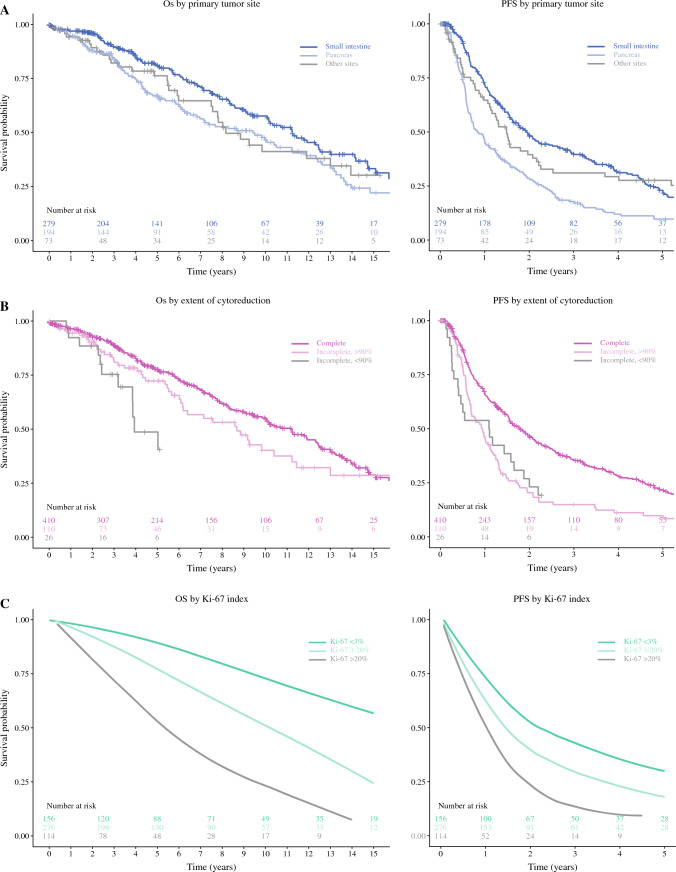
Results: The inclusion criteria were met by 546 patients. The most common primary sites were the small intestine (n = 279) and the pancreas (n = 194). Simultaneous primary tumor resection was performed for 60 % of the cases. Major hepatectomy comprised 27% of the cases, but this rate decreased during the study period (p < 0.001). Major complications occurred in 20%, and the 90-day mortality rate was 1.6%. Functional disease was present in 37 %, and symptomatic relief was achieved in 96%. The median symptom-free interval was 41 months (62 months after complete cytoreduction and 21 months with gross residual disease) (p = 0.021). The median overall survival was 122 months, and progression-free survival was 17 months. In the multivariable analysis, worse overall survival was associated with age, pancreatic primary tumor, Ki-67, number and size of lesions, and extrahepatic metastases, with Ki-67 as the strongest predictor (odds ratio [OR], 1.90 for Ki-67 [3-20%; p = 0.018] and OR, 4.25 for Ki-67 [>20%; p < 0.001]).
Conclusion: The study showed that CRH for NETLMs is associated with low perioperative morbidity and mortality and excellent overall survival, although the majority will experience recurrence/progression. For patients with functional tumors, CRH can provide durable symptomatic relief.
© 2023. The Author(s).
Conflict of interest statement
Thorvardur R. Halfdanarson: served on the consulting/advisory board for Ipsen, TerSera, ScioScientific, Curium, Advanced Accelerator Applications (a Novartis company), Terumo, ITM Isotopen Technologien Muenchen, and Crinetics. Dr Halfdanardson received research support from Thermo Fisher Scientific, Advanced Accelerator Applications (a Novartis company), Basilea, Turnstone Biologics, and Agios. The remaining authors have no conflicts of interest.
Figures
Comment in
-
ASO Author Reflections: Long-Term Outcomes after Cytoreductive Hepatectomy for Neuroendocrine Tumor Liver Metastases.Ann Surg Oncol. 2023 Aug;30(8):4852-4853. doi: 10.1245/s10434-023-13374-x. Epub 2023 Mar 20. Ann Surg Oncol. 2023. PMID: 36940040 No abstract available.
-
Residual Tumor Volume, Not Percent Cytoreduction, Matters for Surgery of Neuroendocrine Liver Metastasis.Ann Surg Oncol. 2023 Sep;30(9):5457-5458. doi: 10.1245/s10434-023-13834-4. Epub 2023 Jul 2. Ann Surg Oncol. 2023. PMID: 37394668 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
