

SUCCOR Nodes: May Sentinel Node Biopsy Determine the Need for Adjuvant Treatment?
- PMID: 37208571
- PMCID: PMC10319697
- DOI: 10.1245/s10434-023-13529-w
SUCCOR Nodes: May Sentinel Node Biopsy Determine the Need for Adjuvant Treatment?
Abstract
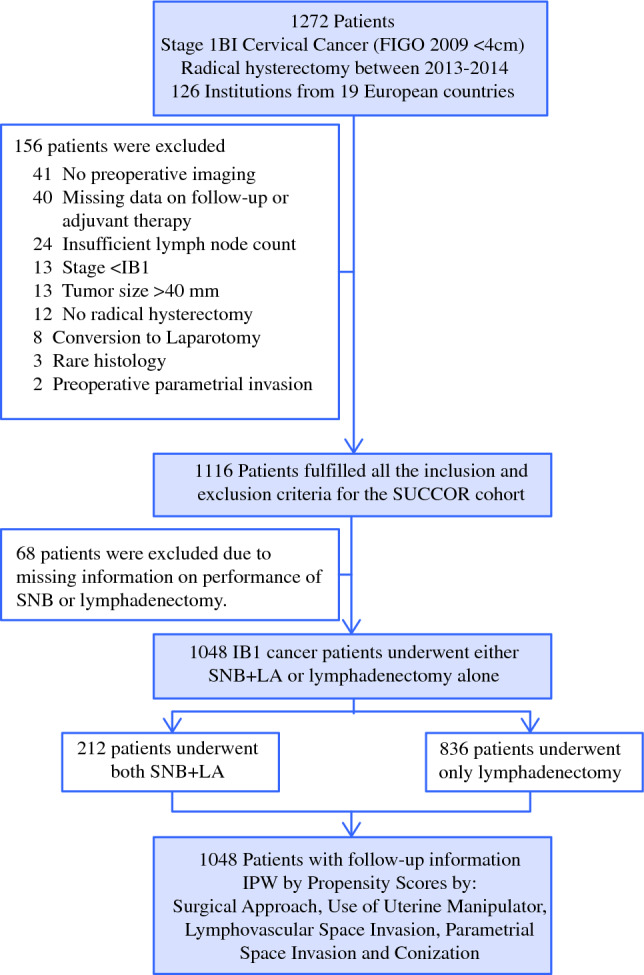
Background: The SUCCOR cohort was developed to analyse the overall and disease-free survival at 5 years in women with FIGO 2009 stage IB1 cervical cancer. The aim of this study was to compare the use of adjuvant therapy in these women, depending on the method used to diagnose lymphatic node metastasis.
Patients and methods: We used data from the SUCCOR cohort, which collected information from 1049 women with FIGO 2009 stage IB1 cervical cancer who were operated on between January 2013 and December 2014 in Europe. We calculated the adjusted proportion of women who received adjuvant therapy depending on the lymph node diagnosis method and compared disease free and overall survival using Cox proportional-hazards regression models. Inverse probability weighting was used to adjust for baseline potential confounders.
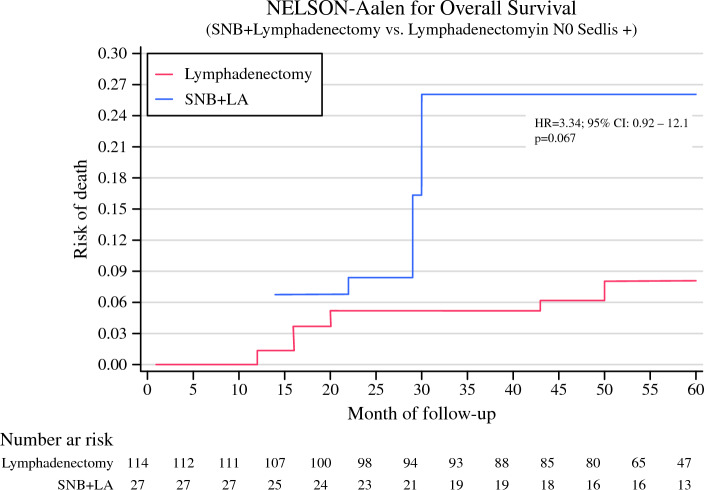
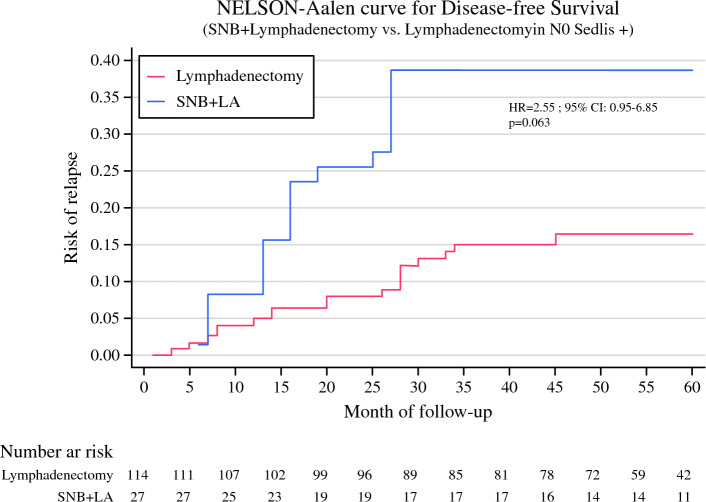
Results: The adjusted proportion of women who received adjuvant therapy was 33.8% in the sentinel node biopsy + lymphadenectomy (SNB+LA) group and 44.7% in the LA group (p = 0.02), although the proportion of positive nodal status was similar (p = 0.30). That difference was greater in women with negative nodal status and positive Sedlis criteria (difference 31.2%, p = 0.01). Here, those who underwent a SNB+LA had an increased risk of relapse [hazard ratio (HR) 2.49, 95% confidence interval (CI) 0.98-6.33, p = 0.056] and risk of death (HR 3.49, 95% CI 1.04-11.7, p = 0.042) compared with those who underwent LA.
Conclusions: Women in this study were less likely to receive adjuvant therapy if their nodal invasion was determined using SNB+LA compared with LA. These results suggest a lack of therapeutic measures available when a negative result is obtained by SNB+LA, which may have an impact on the risk of recurrence and survival.
© 2023. The Author(s).
Conflict of interest statement
All the authors declare no conflict of interest.
Figures
References
-
- Gómez-Hidalgo NR, Acosta Ú, Rodríguez TG, et al. Adjuvant therapy in early-stage cervical cancer after radical hysterectomy: are we overtreating our patients? A meta-analysis. Clin Transl Oncol. 2022;(0123456789). - PubMed
-
- Cibula D, Pötter R, Planchamp F, et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology Guidelines for the Management of Patients With Cervical Cancer. Int J Gynecol Cancer. 2018;28(4):641–655. doi: 10.1097/IGC.0000000000001216. - DOI - PubMed
