

Long-term outcome of COVID-19 patients treated with helmet noninvasive ventilation vs. high-flow nasal oxygen: a randomized trial
- PMID: 37208787
- PMCID: PMC10195662
- DOI: 10.1186/s40560-023-00669-0
Long-term outcome of COVID-19 patients treated with helmet noninvasive ventilation vs. high-flow nasal oxygen: a randomized trial
Abstract
Background: Long-term outcomes of patients treated with helmet noninvasive ventilation (NIV) are unknown: safety concerns regarding the risk of patient self-inflicted lung injury and delayed intubation exist when NIV is applied in hypoxemic patients. We assessed the 6-month outcome of patients who received helmet NIV or high-flow nasal oxygen for COVID-19 hypoxemic respiratory failure.
Methods: In this prespecified analysis of a randomized trial of helmet NIV versus high-flow nasal oxygen (HENIVOT), clinical status, physical performance (6-min-walking-test and 30-s chair stand test), respiratory function and quality of life (EuroQoL five dimensions five levels questionnaire, EuroQoL VAS, SF36 and Post-Traumatic Stress Disorder Checklist for the DSM) were evaluated 6 months after the enrollment.
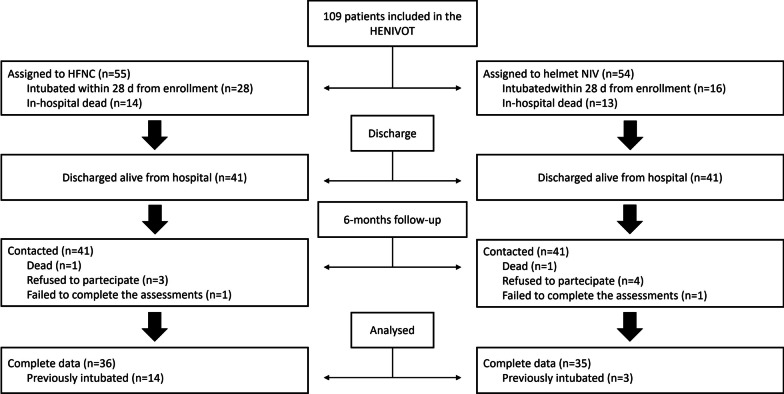
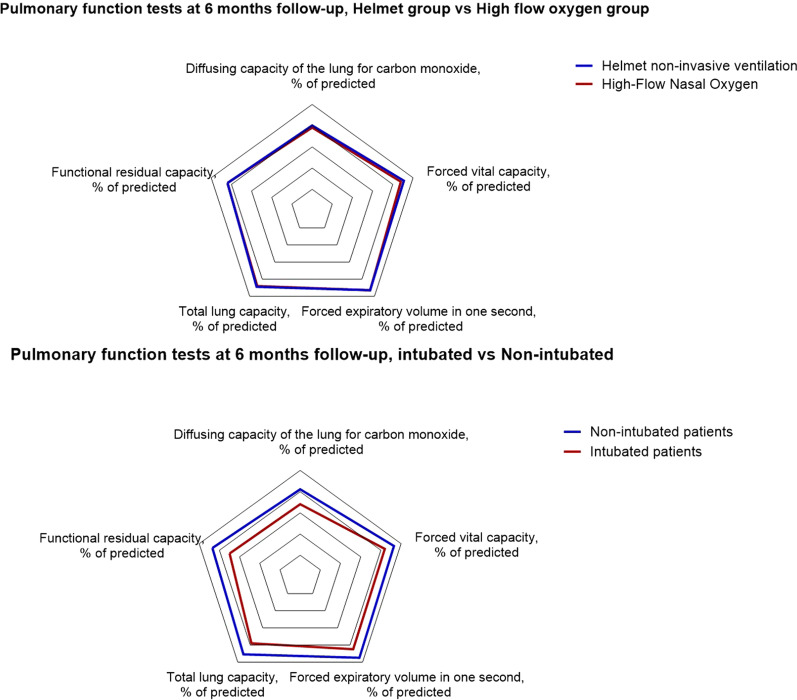
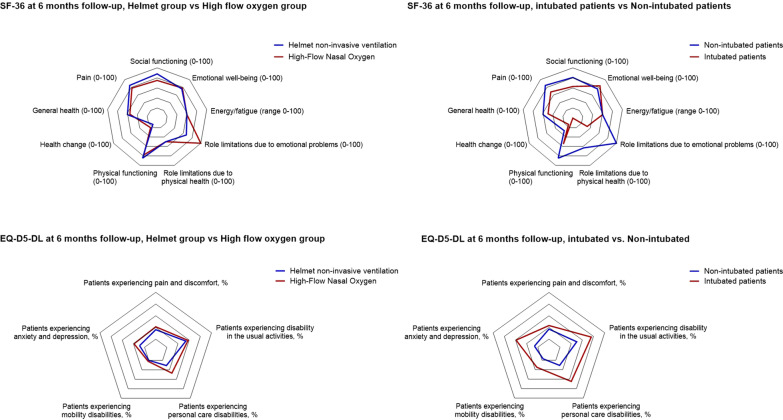
Results: Among 80 patients who were alive, 71 (89%) completed the follow-up: 35 had received helmet NIV, 36 high-flow oxygen. There was no inter-group difference in any item concerning vital signs (N = 4), physical performance (N = 18), respiratory function (N = 27), quality of life (N = 21) and laboratory tests (N = 15). Arthralgia was significantly lower in the helmet group (16% vs. 55%, p = 0.002). Fifty-two percent of patients in helmet group vs. 63% of patients in high-flow group had diffusing capacity of the lungs for carbon monoxide < 80% of predicted (p = 0.44); 13% vs. 22% had forced vital capacity < 80% of predicted (p = 0.51). Both groups reported similar degree of pain (p = 0.81) and anxiety (p = 0.81) at the EQ-5D-5L test; the EQ-VAS score was similar in the two groups (p = 0.27). Compared to patients who successfully avoided invasive mechanical ventilation (54/71, 76%), intubated patients (17/71, 24%) had significantly worse pulmonary function (median diffusing capacity of the lungs for carbon monoxide 66% [Interquartile range: 47-77] of predicted vs. 80% [71-88], p = 0.005) and decreased quality of life (EQ-VAS: 70 [53-70] vs. 80 [70-83], p = 0.01).
Conclusions: In patients with COVID-19 hypoxemic respiratory failure, treatment with helmet NIV or high-flow oxygen yielded similar quality of life and functional outcome at 6 months. The need for invasive mechanical ventilation was associated with worse outcomes. These data indicate that helmet NIV, as applied in the HENIVOT trial, can be safely used in hypoxemic patients. Trial registration Registered on clinicaltrials.gov NCT04502576 on August 6, 2020.
Keywords: Acute respiratory failure; COVID-19; Helmet; High-flow nasal oxygen; Noninvasive ventilation; Patient self-inflicted lung injury (P-SILI).
© 2023. The Author(s).
Conflict of interest statement
DLG has received payments for travel expenses by Getinge and Air Liquide, speaking fees by Intersurgical, GE, Fisher and Paykel, and Gilead. MA has received payments for Board participation from Maquet, Air Liquide, and Chiesi. DLG and MA disclose a research Grant by General Electric Healthcare. DLG is supported by Grants by ESICM and SIAARTI.
Figures
References
-
- Rochwerg B, Brochard L, Elliott MW, Hess D, Hill NS, Nava S, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017. - PubMed
-
- Patel BK, Wolfe KS, Pohlman AS, Hall JB, Kress JP. Effect of noninvasive ventilation delivered by helmet vs. face mask on the rate of endotracheal intubation in patients with acute respiratory distress syndrome a randomized clinical trial. JAMA. 2016;315:2435–2441. doi: 10.1001/jama.2016.6338. - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
