

Motor Activated Auricular Vagus Nerve Stimulation as a Potential Neuromodulation Approach for Post-Stroke Motor Rehabilitation: A Pilot Study
- PMID: 37209010
- PMCID: PMC10363288
- DOI: 10.1177/15459683231173357
Motor Activated Auricular Vagus Nerve Stimulation as a Potential Neuromodulation Approach for Post-Stroke Motor Rehabilitation: A Pilot Study
Abstract
Background: Implanted vagus nerve stimulation (VNS), when synchronized with post-stroke motor rehabilitation improves conventional motor rehabilitation training. A non-invasive VNS method known as transcutaneous auricular vagus nerves stimulation (taVNS) has emerged, which may mimic the effects of implanted VNS.
Objective: To determine whether taVNS paired with motor rehabilitation improves post-stroke motor function, and whether synchronization with movement and amount of stimulation is critical to outcomes.
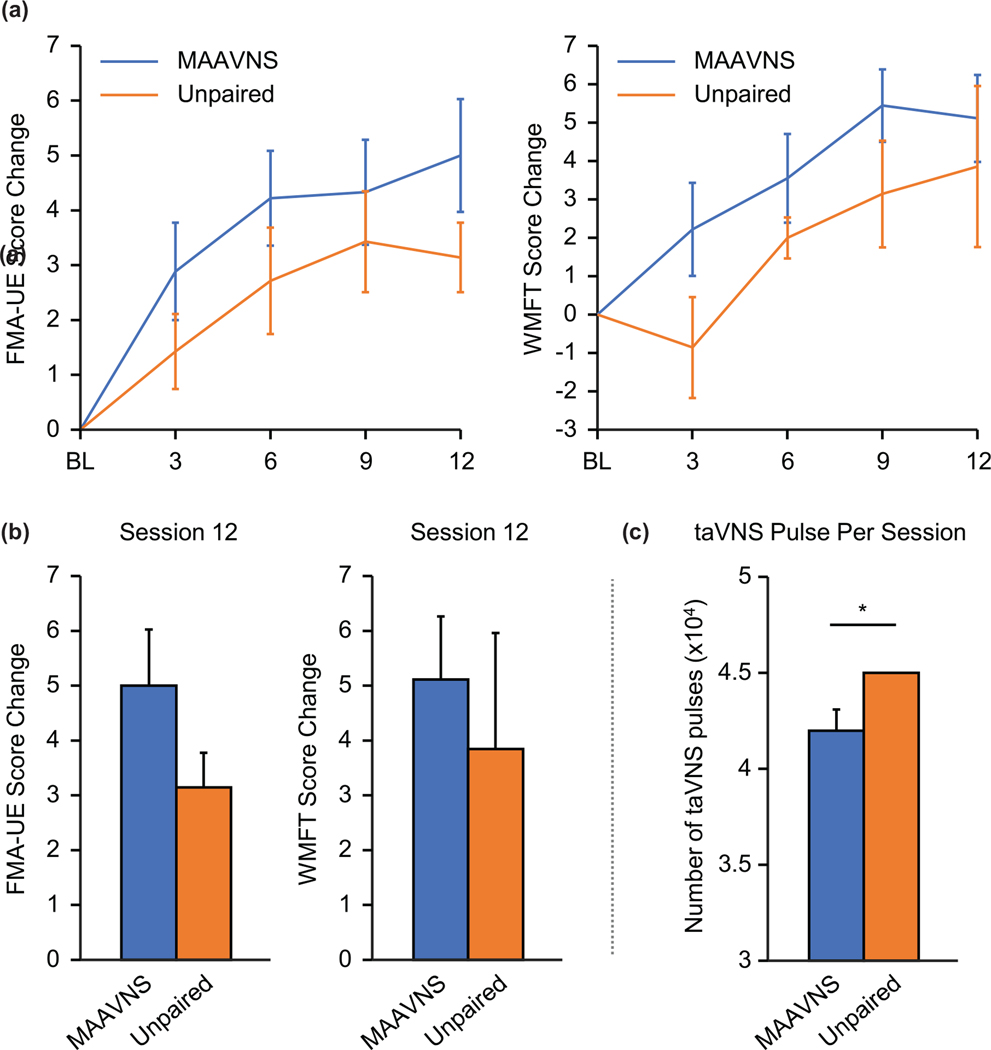
Methods: We developed a closed-loop taVNS system for motor rehabilitation called motor activated auricular vagus nerve stimulation (MAAVNS) and conducted a randomized, double-blind, pilot trial investigating the use of MAAVNS to improve upper limb function in 20 stroke survivors. Participants attended 12 rehabilitation sessions over 4-weeks, and were assigned to a group that received either MAAVNS or active unpaired taVNS concurrently with task-specific training. Motor assessments were conducted at baseline, and weekly during rehabilitation training. Stimulation pulses were counted for both groups.
Results: A total of 16 individuals completed the trial, and both MAAVNS (n = 9) and unpaired taVNS (n = 7) demonstrated improved Fugl-Meyer Assessment upper extremity scores (Mean ± SEM, MAAVNS: 5.00 ± 1.02, unpaired taVNS: 3.14 ± 0.63). MAAVNS demonstrated greater effect size (Cohen's d = 0.63) compared to unpaired taVNS (Cohen's d = 0.30). Furthermore, MAAVNS participants received significantly fewer stimulation pulses (Mean ± SEM, MAAVNS: 36 070 ± 3205) than the fixed 45 000 pulses unpaired taVNS participants received (P < .05).
Conclusion: This trial suggests stimulation timing likely matters, and that pairing taVNS with movements may be superior to an unpaired approach. Additionally, MAAVNS effect size is comparable to that of the implanted VNS approach.
Keywords: MAAVNS; motor activated auricular vagus nerve stimulation; motor rehabilitation; stroke; tVNS; taVNS; transcutaneous auricular vagus nerve stimulation.
Conflict of interest statement
Declaration of Conflicting Interest
All other authors have no conflicts to report.
Figures


References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153–e639. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
