

Effect of modernized collaborative care for depression on depressive symptoms and cardiovascular disease risk biomarkers: eIMPACT randomized controlled trial
- PMID: 37209779
- PMCID: PMC10527905
- DOI: 10.1016/j.bbi.2023.05.007
Effect of modernized collaborative care for depression on depressive symptoms and cardiovascular disease risk biomarkers: eIMPACT randomized controlled trial
Abstract
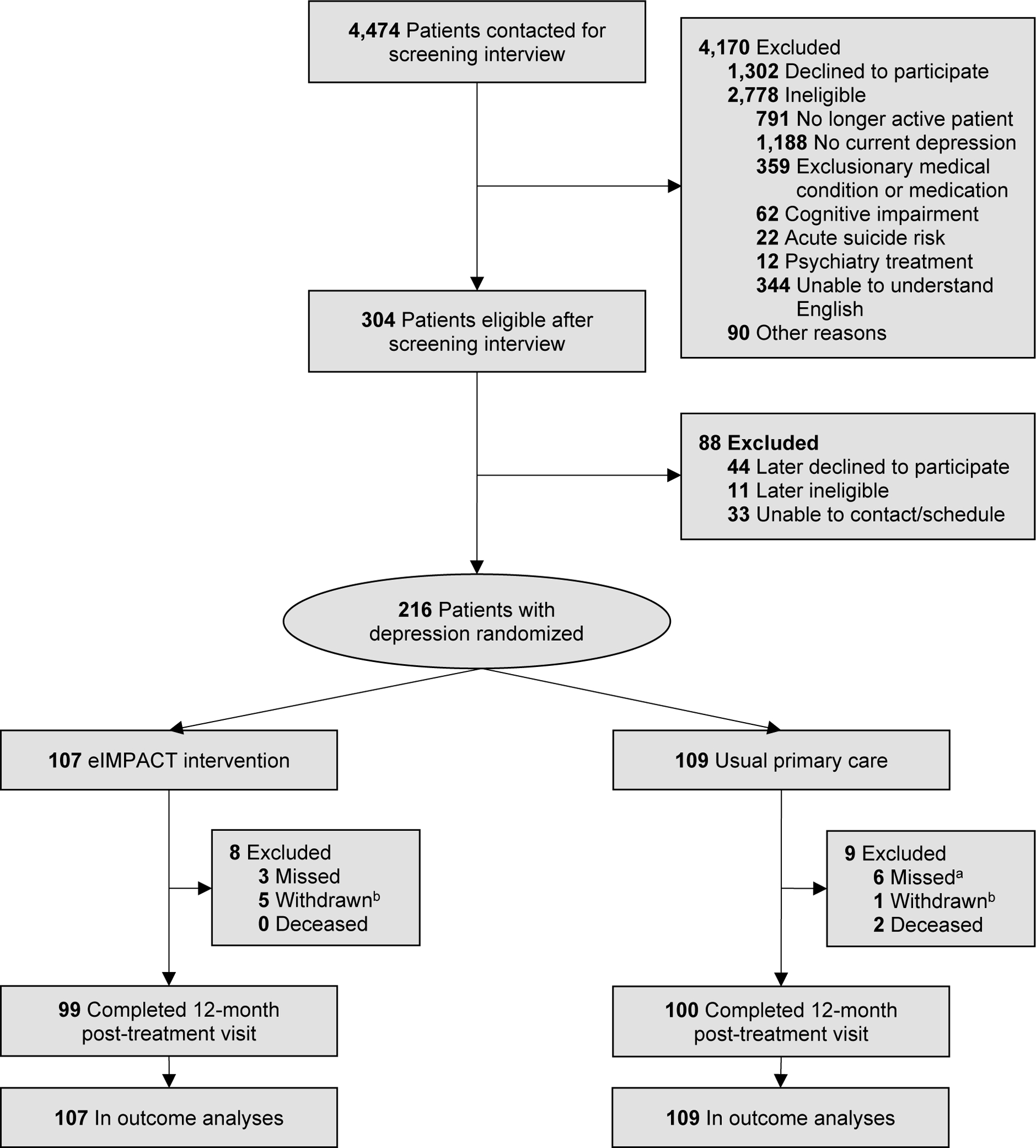
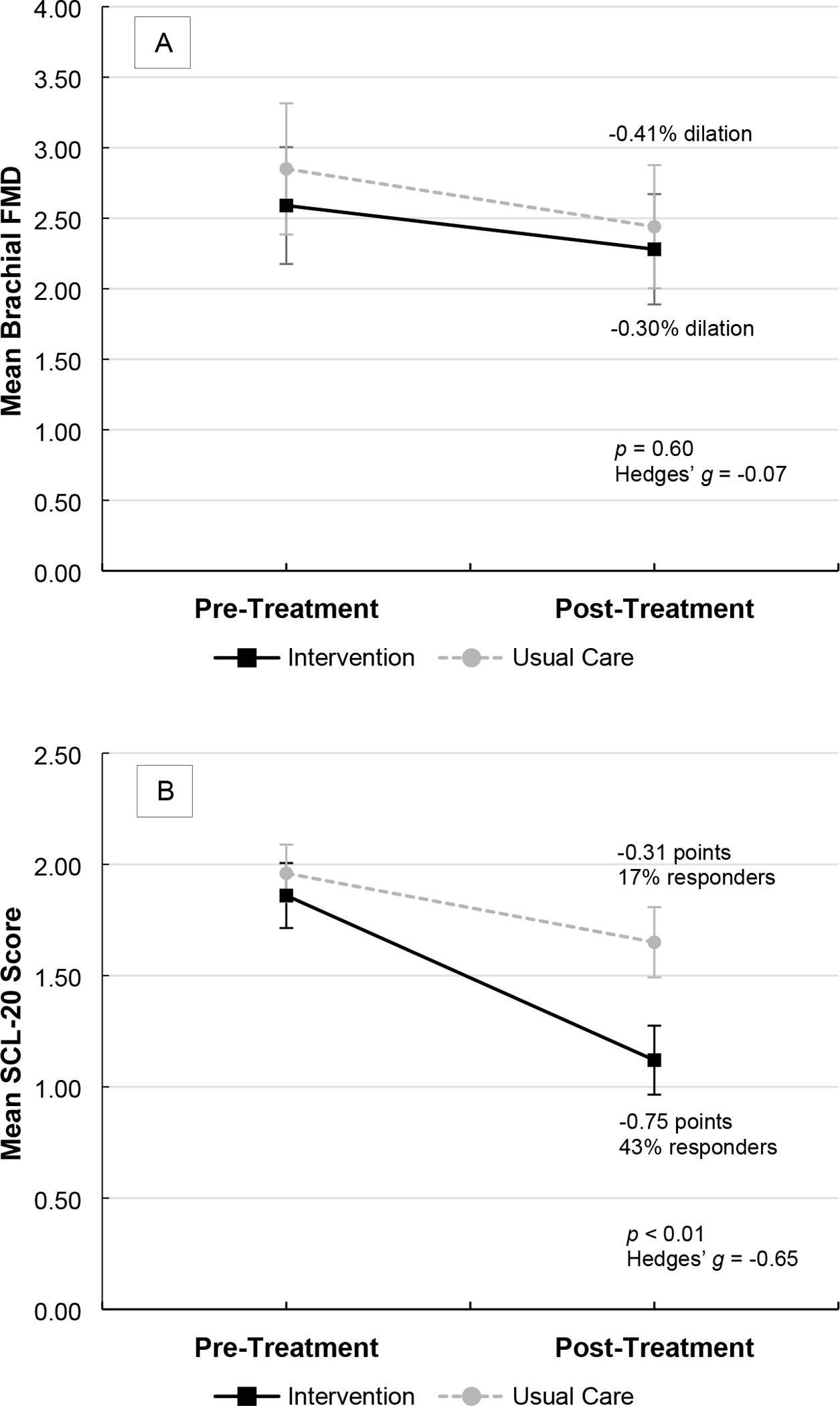
Although depression is a risk and prognostic factor for cardiovascular disease (CVD), clinical trials treating depression in patients with CVD have not demonstrated cardiovascular benefits. We proposed a novel explanation for the null results for CVD-related outcomes: the late timing of depression treatment in the natural history of CVD. Our objective was to determine whether successful depression treatment before, versus after, clinical CVD onset reduces CVD risk in depression. We conducted a single-center, parallel-group, assessor-blinded randomized controlled trial. Primary care patients with depression and elevated CVD risk from a safety net healthcare system (N = 216, Mage = 59 years, 78% female, 50% Black, 46% with income <$10,000/year) were randomized to 12 months of the eIMPACT intervention (modernized collaborative care involving internet cognitive-behavioral therapy [CBT], telephonic CBT, and/or select antidepressants) or usual primary care for depression (primary care providers supported by embedded behavioral health clinicians and psychiatrists). Outcomes were depressive symptoms and CVD risk biomarkers at 12 months. Intervention participants, versus usual care participants, exhibited moderate-to-large (Hedges' g = -0.65, p < 0.01) improvements in depressive symptoms. Clinical response data yielded similar results - 43% of intervention participants, versus 17% of usual care participants, had a ≥ 50% reduction in depressive symptoms (OR = 3.73, 95% CI: 1.93-7.21, p < 0.01). However, no treatment group differences were observed for the CVD risk biomarkers - i.e., brachial flow-mediated dilation, high-frequency heart rate variability, interleukin-6, high-sensitivity C-reactive protein, β-thromboglobulin, and platelet factor 4 (Hedges' gs = -0.23 to 0.02, ps ≥ 0.09). Our modernized collaborative care intervention - which harnessed technology to maximize access and minimize resources - produced clinically meaningful improvements in depressive symptoms. However, successful depression treatment did not lower CVD risk biomarkers. Our findings indicate that depression treatment alone may not be sufficient to reduce the excess CVD risk of people with depression and that alternative approaches are needed. In addition, our effective intervention highlights the utility of eHealth interventions and centralized, remote treatment delivery in safety net clinical settings and could inform contemporary integrated care approaches. Trial Registration:ClinicalTrials.gov Identifier: NCT02458690.
Keywords: Autonomic dysfunction; Cardiovascular disease; Clinical trial; Collaborative care; Depression; Endothelial dysfunction; Internet interventions; Platelet activation; Systemic inflammation.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: The authors have no potential conflicts of interest to declare related to the subject matter of this article. Several authors (J.C.S., B.M.P., S.G., J.I.N., S.K.G., R.V.C., B.L.R., C.M.C.) received grants from the NIH. J.C.S. received advisory fees from Boston Medical Center. J.I.N. received support as an investigator from Janssen. S.K.G. received advisory fees from Gilead Sciences and ViiV Healthcare and grants from ViiV Healthcare. R.V.C. received grants from Almond Board of California, American Diabetes Association, and Eli Lilly and Company.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
