

Phase II trial of fulvestrant plus enzalutamide in ER+/HER2- advanced breast cancer
- PMID: 37210417
- PMCID: PMC10199936
- DOI: 10.1038/s41523-023-00544-z
Phase II trial of fulvestrant plus enzalutamide in ER+/HER2- advanced breast cancer
Abstract
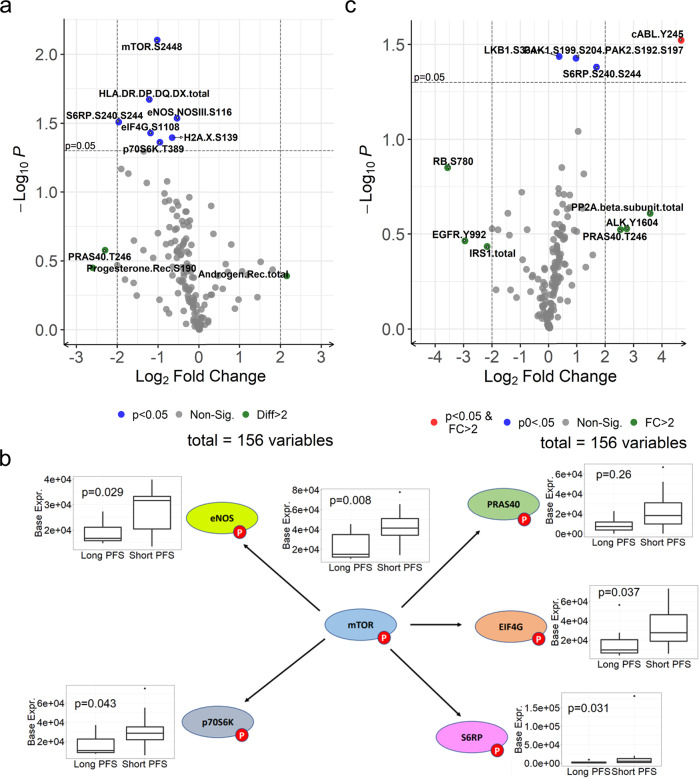
This clinical trial combined fulvestrant with the anti-androgen enzalutamide in women with metastatic ER+/HER2- breast cancer (BC). Eligible patients were women with ECOG 0-2, ER+/HER2- measurable or evaluable metastatic BC. Prior fulvestrant was allowed. Fulvestrant was administered at 500 mg IM on days 1, 15, 29, and every 4 weeks thereafter. Enzalutamide was given at 160 mg po daily. Fresh tumor biopsies were required at study entry and after 4 weeks of treatment. The primary efficacy endpoint of the trial was the clinical benefit rate at 24 weeks (CBR24). The median age was 61 years (46-87); PS 1 (0-1); median of 4 prior non-hormonal and 3 prior hormonal therapies for metastatic disease. Twelve had prior fulvestrant, and 91% had visceral disease. CBR24 was 25% (7/28 evaluable). Median progression-free survival (PFS) was 8 weeks (95% CI: 2-52). Adverse events were as expected for hormonal therapy. Significant (p < 0.1) univariate relationships existed between PFS and ER%, AR%, and PIK3CA and/or PTEN mutations. Baseline levels of phospho-proteins in the mTOR pathway were more highly expressed in biopsies of patients with shorter PFS. Fulvestrant plus enzalutamide had manageable side effects. The primary endpoint of CBR24 was 25% in heavily pretreated metastatic ER+/HER2- BC. Short PFS was associated with activation of the mTOR pathway, and PIK3CA and/or PTEN mutations were associated with an increased hazard of progression. Thus, a combination of fulvestrant or other SERD plus AKT/PI3K/mTOR inhibitor with or without AR inhibition warrants investigation in second-line endocrine therapy of metastatic ER+ BC.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
