

Patient Preferences Regarding Surgical Treatment Methods for Symptomatic Uterine Fibroids
- PMID: 37210440
- PMCID: PMC10400705
- DOI: 10.1007/s43441-023-00525-1
Patient Preferences Regarding Surgical Treatment Methods for Symptomatic Uterine Fibroids
Abstract
Study objective: The purpose of this study is to rank the factors that are most and least important to patients with symptomatic uterine fibroids when considering surgical treatment options.
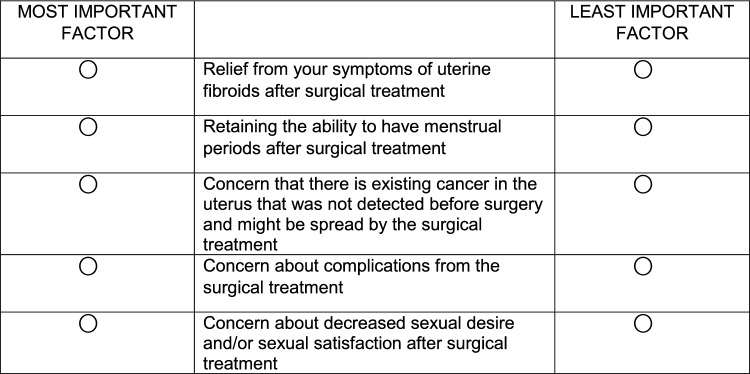
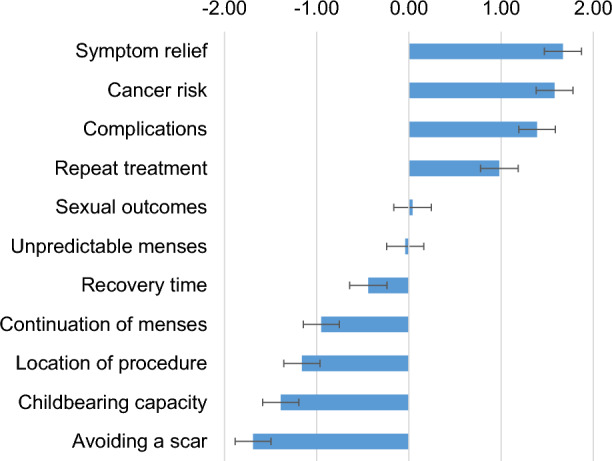
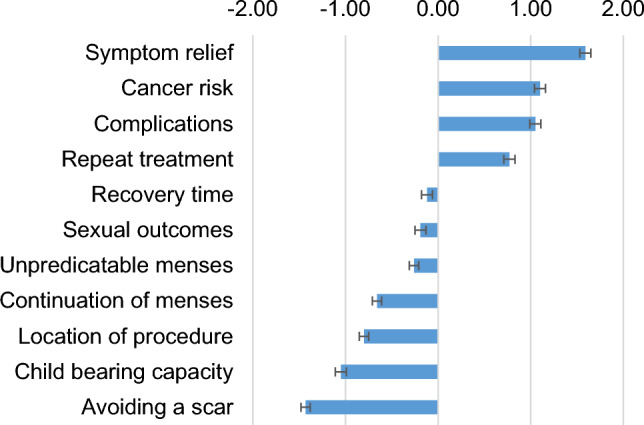
Materials and methods: Using a best worst scaling (BWS) preference elicitation approach, participants completed an online survey to rank factors associated with fibroid surgical treatments. Survey content was based on a literature review and included the following factors: symptom relief; surgical complications; repeat treatment; recovery time; cosmetic effects; risk of spreading undiagnosed cancer; sexual outcomes; maintenance of child-bearing; continuation of menses; unpredictable menses; and location of procedure. Participants completed 11 BWS tasks. For each task, we presented participants with a subset of 5 factors from the possible 11, and participants chose the most important and least important factor. Participants' responses were analyzed using conditional logistic regression to determine the relative importance of factors. Patient priorities were further explored via age and race.
Results: 285 respondents with symptomatic uterine fibroids (69 physician-confirmed and 216 self-reported) who had not undergone prior surgical treatment completed the survey. Respondents were enrolled from two clinical sites (clinical site cohort) and an online consumer panel (panel cohort). Both cohorts identified symptom relief, cancer risk, repeat treatment and complications as the most important factors in selecting surgical treatment options and location of procedure, return to normal activities after surgery, and cosmetic effects like presence of a scar after the surgical treatment as the least important factors. Of note, younger women (≤ 40) placed greater importance on the ability to have children after the procedure.
Conclusion: Information regarding the factors most and least important to patients with symptomatic uterine fibroids might inform development and regulatory evaluation of new technologies and procedures. Study results may be useful in efforts to develop a set of outcomes to include in future fibroids clinical studies.
Keywords: Benefit-risk assessment; Best Worst Scaling; Patient preferences; Patient priorities; Product development; Uterine fibroids.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
