

Intervention to Promote Communication About Goals of Care for Hospitalized Patients With Serious Illness: A Randomized Clinical Trial
- PMID: 37210665
- PMCID: PMC10201405
- DOI: 10.1001/jama.2023.8812
Intervention to Promote Communication About Goals of Care for Hospitalized Patients With Serious Illness: A Randomized Clinical Trial
Erratum in
-
Incorrect Text in Discussion Section.JAMA. 2023 Sep 5;330(9):880. doi: 10.1001/jama.2023.15610. JAMA. 2023. PMID: 37668636 Free PMC article. No abstract available.
Abstract
Importance: Discussions about goals of care are important for high-quality palliative care yet are often lacking for hospitalized older patients with serious illness.
Objective: To evaluate a communication-priming intervention to promote goals-of-care discussions between clinicians and hospitalized older patients with serious illness.
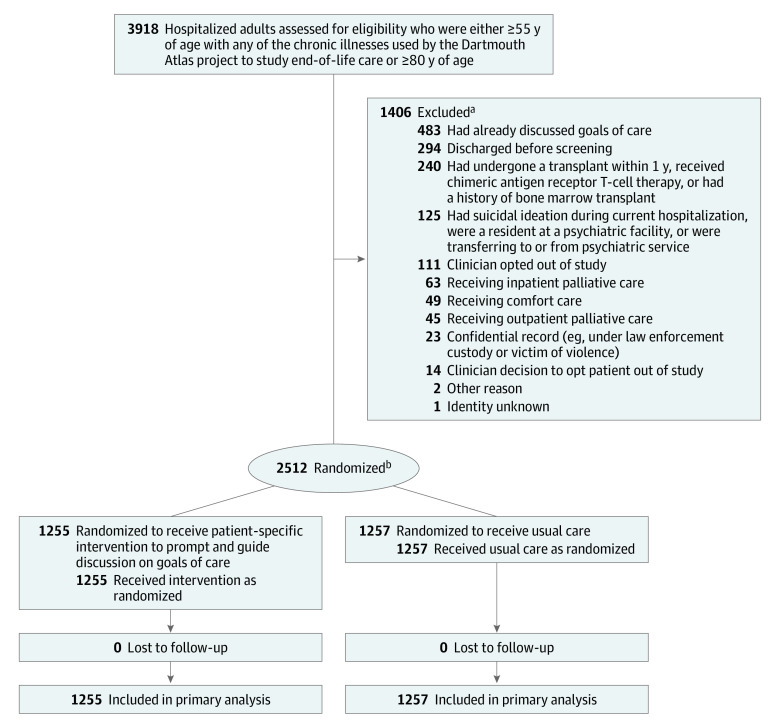
Design, setting, and participants: A pragmatic, randomized clinical trial of a clinician-facing communication-priming intervention vs usual care was conducted at 3 US hospitals within 1 health care system, including a university, county, and community hospital. Eligible hospitalized patients were aged 55 years or older with any of the chronic illnesses used by the Dartmouth Atlas project to study end-of-life care or were aged 80 years or older. Patients with documented goals-of-care discussions or a palliative care consultation between hospital admission and eligibility screening were excluded. Randomization occurred between April 2020 and March 2021 and was stratified by study site and history of dementia.
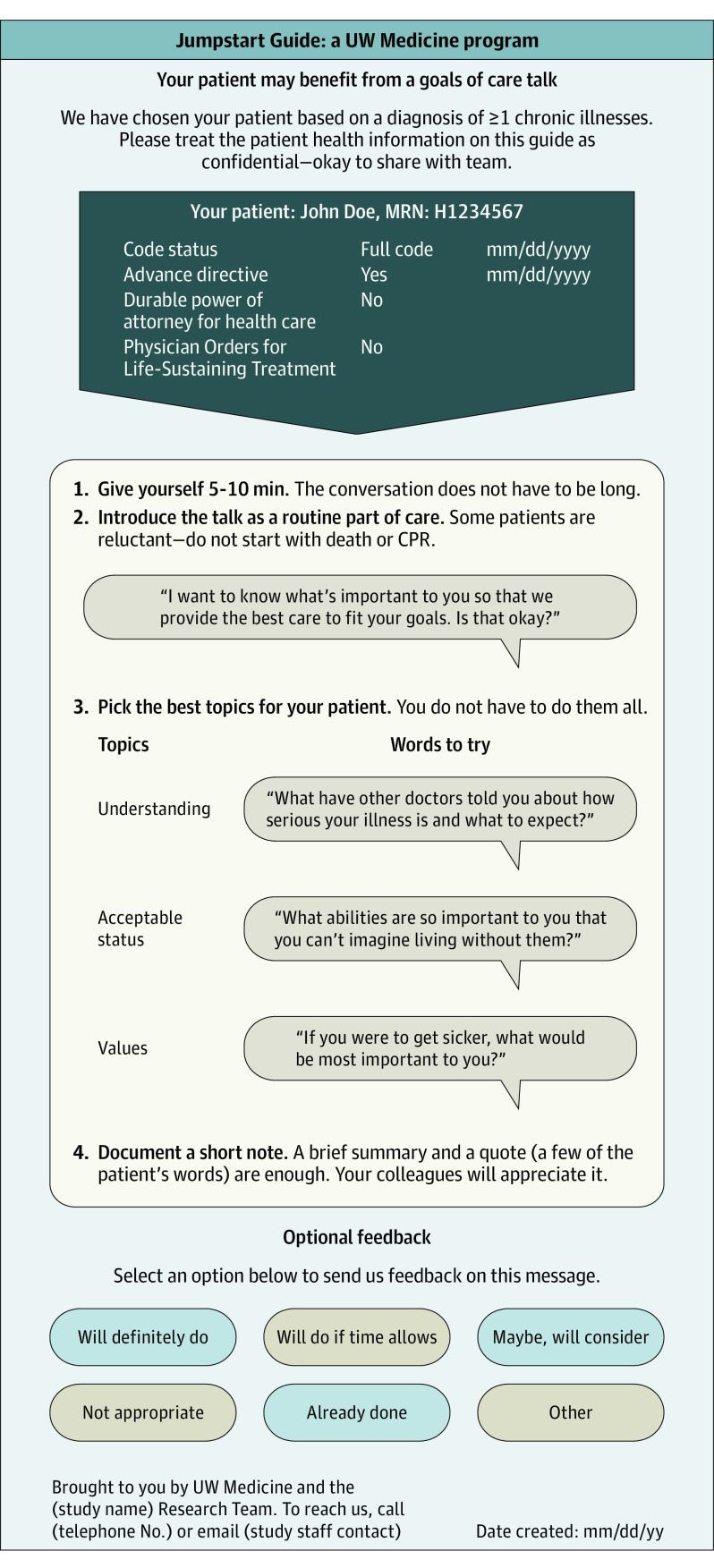
Intervention: Physicians and advance practice clinicians who were treating the patients randomized to the intervention received a 1-page, patient-specific intervention (Jumpstart Guide) to prompt and guide goals-of-care discussions.
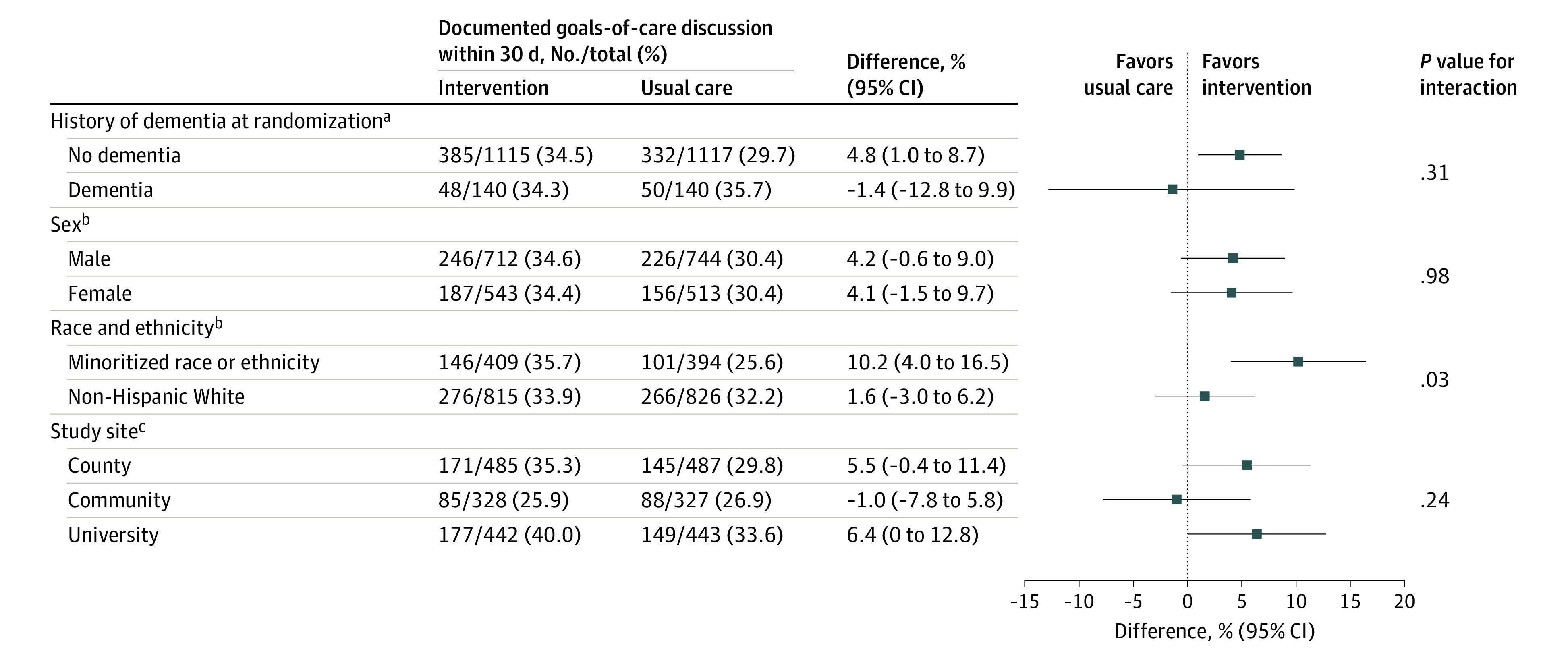
Main outcomes and measures: The primary outcome was the proportion of patients with electronic health record-documented goals-of-care discussions within 30 days. There was also an evaluation of whether the effect of the intervention varied by age, sex, history of dementia, minoritized race or ethnicity, or study site.
Results: Of 3918 patients screened, 2512 were enrolled (mean age, 71.7 [SD, 10.8] years and 42% were women) and randomized (1255 to the intervention group and 1257 to the usual care group). The patients were American Indian or Alaska Native (1.8%), Asian (12%), Black (13%), Hispanic (6%), Native Hawaiian or Pacific Islander (0.5%), non-Hispanic (93%), and White (70%). The proportion of patients with electronic health record-documented goals-of-care discussions within 30 days was 34.5% (433 of 1255 patients) in the intervention group vs 30.4% (382 of 1257 patients) in the usual care group (hospital- and dementia-adjusted difference, 4.1% [95% CI, 0.4% to 7.8%]). The analyses of the treatment effect modifiers suggested that the intervention had a larger effect size among patients with minoritized race or ethnicity. Among 803 patients with minoritized race or ethnicity, the hospital- and dementia-adjusted proportion with goals-of-care discussions was 10.2% (95% CI, 4.0% to 16.5%) higher in the intervention group than in the usual care group. Among 1641 non-Hispanic White patients, the adjusted proportion with goals-of-care discussions was 1.6% (95% CI, -3.0% to 6.2%) higher in the intervention group than in the usual care group. There was no evidence of differential treatment effects of the intervention on the primary outcome by age, sex, history of dementia, or study site.
Conclusions and relevance: Among hospitalized older adults with serious illness, a pragmatic clinician-facing communication-priming intervention significantly improved documentation of goals-of-care discussions in the electronic health record, with a greater effect size in racially or ethnically minoritized patients.
Trial registration: ClinicalTrials.gov Identifier: NCT04281784.
Conflict of interest statement
Figures
Comment in
-
Conversations on Goals of Care With Hospitalized, Seriously Ill Patients.JAMA. 2023 Jun 20;329(23):2021-2022. doi: 10.1001/jama.2023.8970. JAMA. 2023. PMID: 37210664 No abstract available.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
