

Efficacy of pulmonary artery pressure monitoring in patients with chronic heart failure: a meta-analysis of three randomized controlled trials
- PMID: 37210750
- PMCID: PMC10542655
- DOI: 10.1093/eurheartj/ehad346
Efficacy of pulmonary artery pressure monitoring in patients with chronic heart failure: a meta-analysis of three randomized controlled trials
Abstract
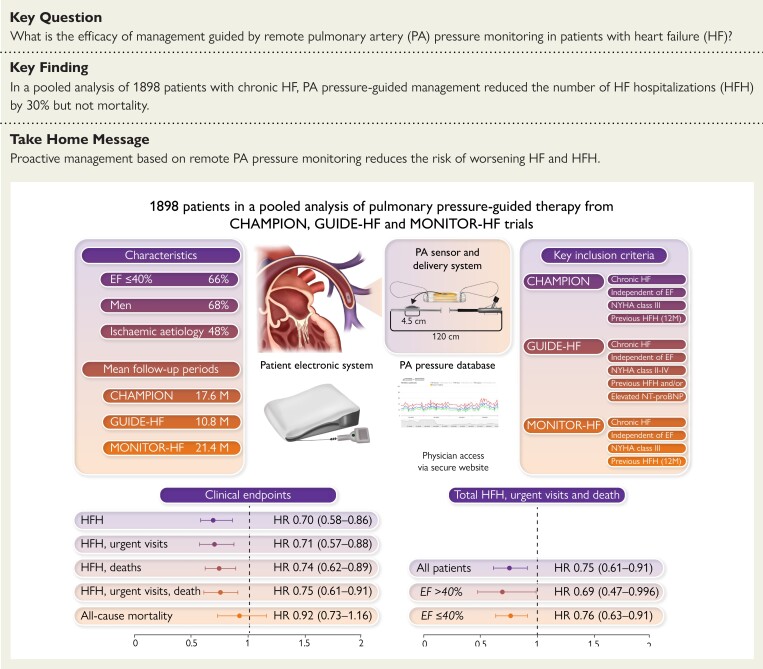
Aims: Adjustment of treatment based on remote monitoring of pulmonary artery (PA) pressure may reduce the risk of hospital admission for heart failure (HF). We have conducted a meta-analysis of large randomized trials investigating this question.
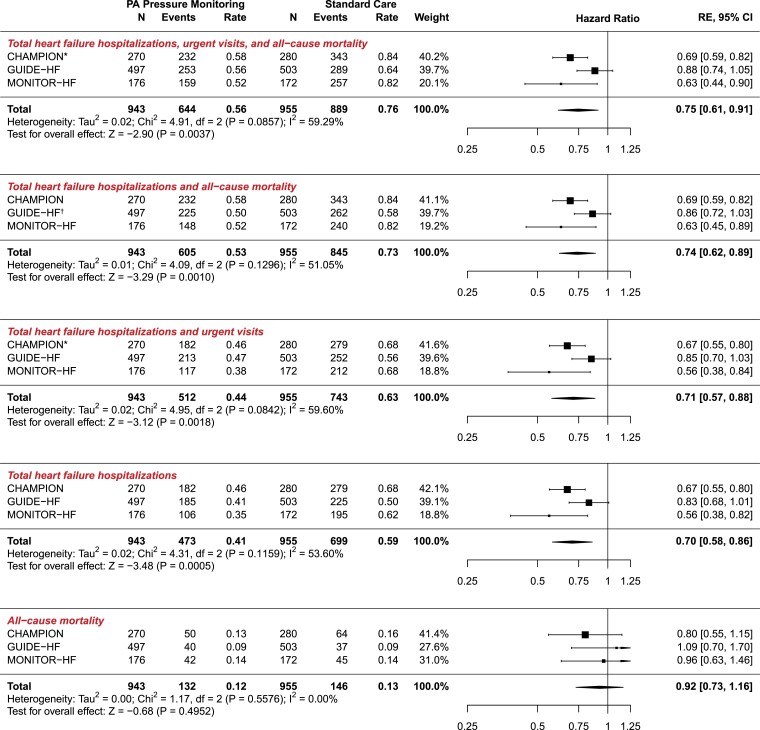
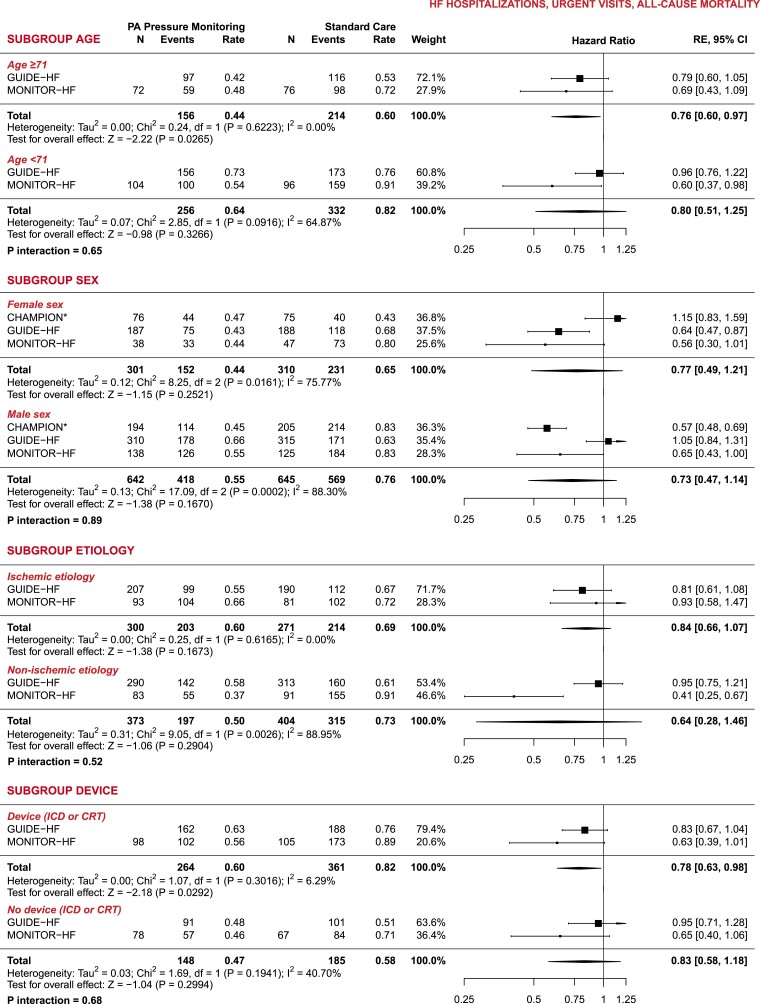
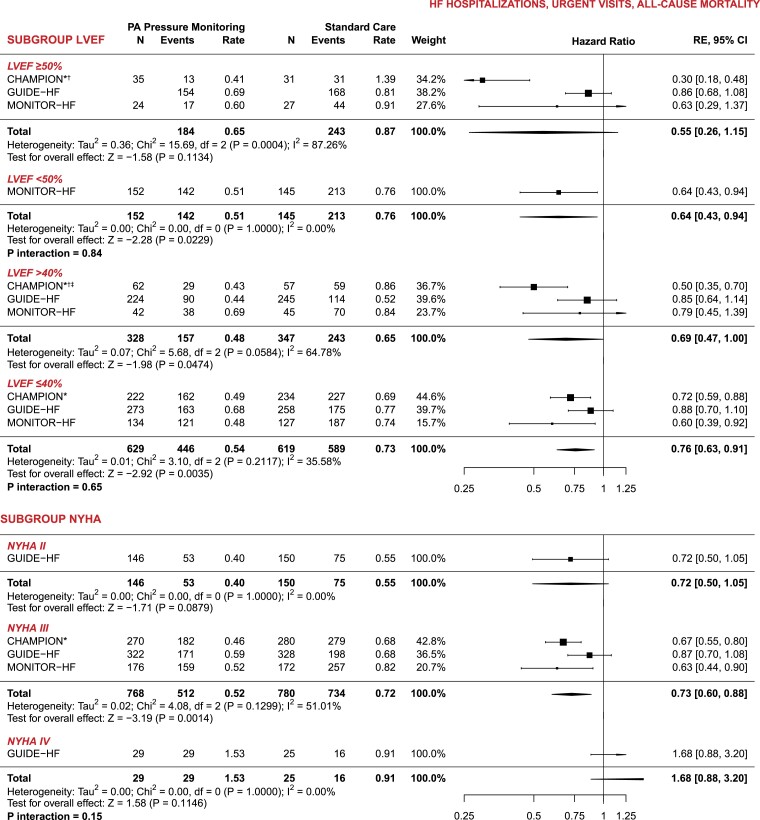
Methods and results: A systematic literature search was performed for randomized clinical trials with PA pressure monitoring devices in patients with HF. The primary outcome of interest was the total number of HF hospitalizations. Other outcomes assessed were urgent visits leading to treatment with intravenous diuretics, all-cause mortality, and composites. Treatment effects are expressed as hazard ratios, and pooled effect estimates were obtained applying random effects meta-analyses. Three eligible randomized clinical trials were identified that included 1898 outpatients in New York Heart Association functional classes II-IV, either hospitalized for HF in the prior 12 months or with elevated plasma NT-proBNP concentrations. The mean follow-up was 14.7 months, 67.8% of the patients were men, and 65.8% had an ejection fraction ≤40%. Compared to patients in the control group, the hazard ratio (95% confidence interval) for total HF hospitalizations in those randomized to PA pressure monitoring was 0.70 (0.58-0.86) (P = .0005). The corresponding hazard ratio for the composite of total HF hospitalizations, urgent visits and all-cause mortality was 0.75 (0.61-0.91; P = .0037) and for all-cause mortality 0.92 (0.73-1.16). Subgroup analyses, including ejection fraction phenotype, revealed no evidence of heterogeneity in the treatment effect.
Conclusion: The use of remote PA pressure monitoring to guide treatment of patients with HF reduces episodes of worsening HF and subsequent hospitalizations.
Keywords: Heart failure; Monitoring; Pulmonary artery pressure; Sensor; Trial.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest P.R.D.C., S.P.R., E.B. report no conflict of interest to declare. R.A.d.B. has received research grants and/or fees from AstraZeneca, Abbott, Boehringer Ingelheim, Cardior Pharmaceuticals GmbH, Ionis Pharmaceuticals, Inc., Novo Nordisk, and Roche; and has had speaker engagements with Abbott, AstraZeneca, Bayer, Bristol Myers Squibb, Novartis, and Roche. J.G. has received consulting fees from Applied Therapeutics, Amarin, Boehringer-Ingelheim, Biosensors, Cardialysis, Edwards Lifesciences, MVRx and Whiteswell and reimbursement of travel expenses from Abbott. W.T.A. has received personal fees from Abbott, Boehringer-Ingelheim, Edwards Lifesciences, Impulse Dynamics, Sensible Medical, Vectorious Medical Technolgoies, V-Wave Medical, and Zoll Respicardia. P.S.J. received consulting fees, advisory board fees and lecture fees from Novartis; advisory board fees from Cytokinetics; and grant support from Boehringer Ingelheim. J.J.V.M.M. received payments through Glasgow University from work on clinical trials, consulting and other activities from Alnylam, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Cardurion, Cytokinetics, DalCor, GSK, KBP Biosciences, Novartis, Pfizer and Theracos, and personal payments from Abbott, Hikma, Ionis, Sun Pharmaceuticals and Servier. J.J.V.M.M. and P.S.J. are supported by a British Heart Foundation Centre of Research Excellence Grant (RE/18/6/34217). J.J.B. received independent research grant from Abbott for ISS and has had speaker engagement or advisory boards in the past 5 years with Astra Zeneca, Abbott, Boehringer-Ingelheim, Bayer, Daiichi Sankyo, Novartis and Vifor.
Figures
Comment in
-
Remote heart failure management guided by pulmonary artery pressure home monitoring: rewriting the future?Eur Heart J. 2023 Oct 1;44(37):3669-3671. doi: 10.1093/eurheartj/ehad525. Eur Heart J. 2023. PMID: 37670404 No abstract available.
References
-
- Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo-Leiro MG, Harjola V-P, et al. . Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC heart failure long-term registry. Eur J Heart Fail 2017;19:1574–1585. 10.1002/ejhf.813 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
