

A machine-learning approach for decision support and risk stratification of pediatric perioperative patients based on the APRICOT dataset
- PMID: 37211981
- PMCID: PMC11485222
- DOI: 10.1111/pan.14694
A machine-learning approach for decision support and risk stratification of pediatric perioperative patients based on the APRICOT dataset
Abstract
Background: Pediatric anesthesia has evolved to a high level of patient safety, yet a small chance remains for serious perioperative complications, even in those traditionally considered at low risk. In practice, prediction of at-risk patients currently relies on the American Society of Anesthesiologists Physical Status (ASA-PS) score, despite reported inconsistencies with this method.
Aims: The goal of this study was to develop predictive models that can classify children as low risk for anesthesia at the time of surgical booking and after anesthetic assessment on the procedure day.
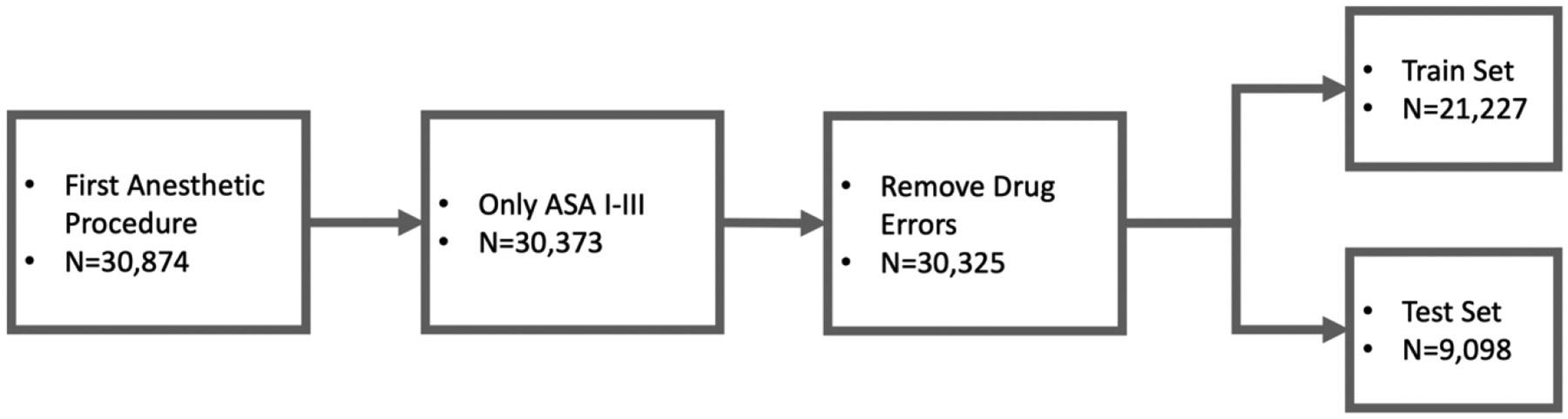
Methods: Our dataset was derived from APRICOT, a prospective observational cohort study conducted by 261 European institutions in 2014 and 2015. We included only the first procedure, ASA-PS classification I to III, and perioperative adverse events not classified as drug errors, reducing the total number of records to 30 325 with an adverse event rate of 4.43%. From this dataset, a stratified train:test split of 70:30 was used to develop predictive machine learning algorithms that could identify children in ASA-PS class I to III at low risk for severe perioperative critical events that included respiratory, cardiac, allergic, and neurological complications.
Results: Our selected models achieved accuracies of >0.9, areas under the receiver operating curve of 0.6-0.7, and negative predictive values >95%. Gradient boosting models were the best performing for both the booking phase and the day-of-surgery phase.
Conclusions: This work demonstrates that prediction of patients at low risk of critical PAEs can be made on an individual, rather than population-based, level by using machine learning. Our approach yielded two models that accommodate wide clinical variability and, with further development, are potentially generalizable to many surgical centers.
Keywords: anesthesia; artificial intelligence; machine learning; pediatrics; preoperative care.
© 2023 John Wiley & Sons Ltd.
Conflict of interest statement
Figures


Comment in
-
Taking a byte out of APRICOT to predict which children are at low risk for critical perioperative events.Paediatr Anaesth. 2023 Sep;33(9):687-688. doi: 10.1111/pan.14707. Epub 2023 Jun 13. Paediatr Anaesth. 2023. PMID: 37309606 No abstract available.
Similar articles
-
Can Predictive Modeling Tools Identify Patients at High Risk of Prolonged Opioid Use After ACL Reconstruction?Clin Orthop Relat Res. 2020 Jul;478(7):0-1618. doi: 10.1097/CORR.0000000000001251. Clin Orthop Relat Res. 2020. PMID: 32282466 Free PMC article.
-
Development and validation of a machine learning ASA-score to identify candidates for comprehensive preoperative screening and risk stratification.J Clin Anesth. 2023 Aug;87:111103. doi: 10.1016/j.jclinane.2023.111103. Epub 2023 Mar 8. J Clin Anesth. 2023. PMID: 36898279
-
Prediction of American Society of Anesthesiologists Physical Status Classification from preoperative clinical text narratives using natural language processing.BMC Anesthesiol. 2023 Sep 4;23(1):296. doi: 10.1186/s12871-023-02248-0. BMC Anesthesiol. 2023. PMID: 37667258 Free PMC article.
-
Machine-learning Models Predict 30-Day Mortality, Cardiovascular Complications, and Respiratory Complications After Aseptic Revision Total Joint Arthroplasty.Clin Orthop Relat Res. 2022 Nov 1;480(11):2137-2145. doi: 10.1097/CORR.0000000000002276. Epub 2022 Jun 20. Clin Orthop Relat Res. 2022. PMID: 35767804 Free PMC article.
-
Machine learning methods for perioperative anesthetic management in cardiac surgery patients: a scoping review.J Thorac Dis. 2021 Dec;13(12):6976-6993. doi: 10.21037/jtd-21-765. J Thorac Dis. 2021. PMID: 35070381 Free PMC article.
Cited by
-
Strengthening Discovery and Application of Artificial Intelligence in Anesthesiology: A Report from the Anesthesia Research Council.Anesthesiology. 2025 Apr 1;142(4):599-610. doi: 10.1097/ALN.0000000000005326. Epub 2025 Mar 11. Anesthesiology. 2025. PMID: 40067037
-
Machine Learning in Pediatric Healthcare: Current Trends, Challenges, and Future Directions.J Clin Med. 2025 Jan 26;14(3):807. doi: 10.3390/jcm14030807. J Clin Med. 2025. PMID: 39941476 Free PMC article. Review.
-
Novel Preoperative Risk Stratification Using Digital Phenotyping Applying a Scalable Machine-Learning Approach.Anesth Analg. 2024 Jul 1;139(1):174-185. doi: 10.1213/ANE.0000000000006753. Epub 2023 Dec 5. Anesth Analg. 2024. PMID: 38051671 Free PMC article.
References
-
- Kurth CD, Tyler D, Heitmiller E, Tosone SR, Martin L, Deshpande JK. National pediatric anesthesia safety quality improvement program in the United States. Anesth Analg. 2014;119(1):112–121. - PubMed
-
- Owens WD. American Society of Anesthesiologists Physical Status Classification System is not a risk classification system. Anesthesiology. 2001;94(2):378–378. - PubMed
-
- Hartley B, Powell S, Bew S. Safe delivery of paediatric ENT surgery in the UK: a national strategy 2019. Accessed [2023-02-14]. https://www.entuk.org/news_and_events/news/77/safe_delivery_of_paediatri...
-
- Whippey A, Kostandoff G, Ma HK, Cheng J, Thabane L, Paul J. Predictors of unanticipated admission following ambulatory surgery in the pediatric population: a retrospective case–control study. Paediatr Anaesth.. 2016;26(8):831–837. - PubMed
-
- Junger A, Klasen J, Benson M, et al. Factors determining length of stay of surgical day-case patients. Eur J Anaesthesiol. 2001;18(5):314–321. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
