

Intramural Healthcare Consumption and Costs After Traumatic Brain Injury: A Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Study
- PMID: 37212277
- PMCID: PMC10541942
- DOI: 10.1089/neu.2022.0429
Intramural Healthcare Consumption and Costs After Traumatic Brain Injury: A Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Study
Abstract
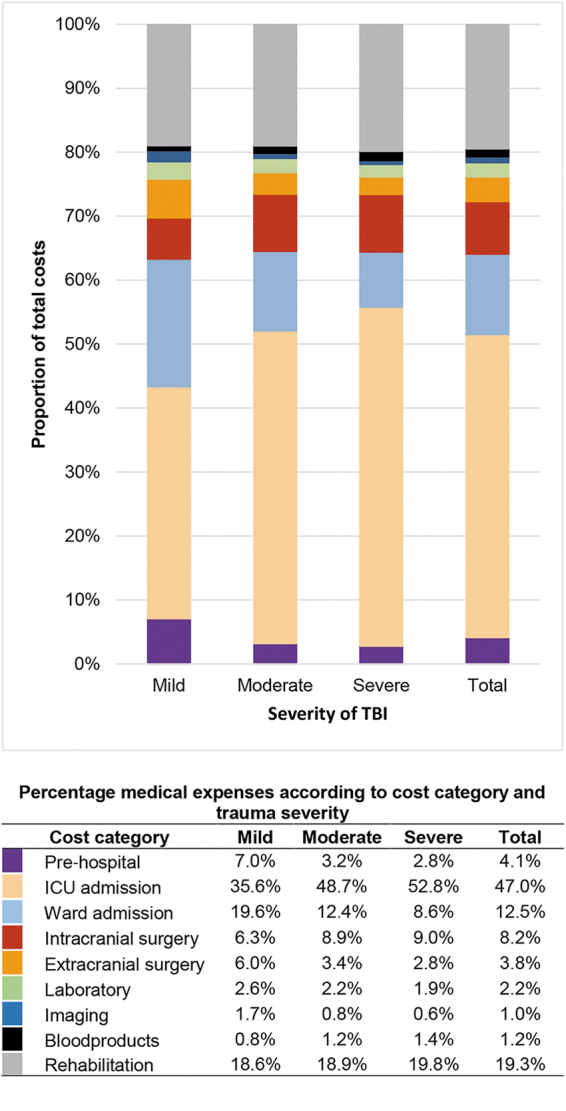
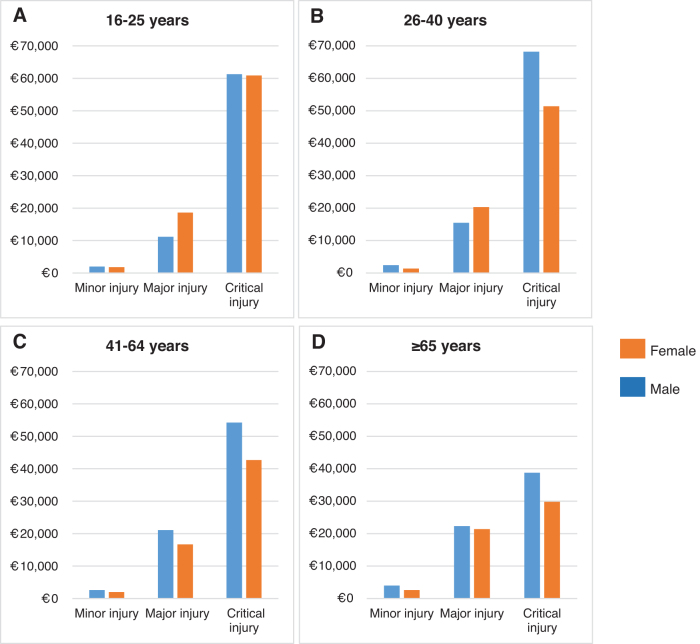
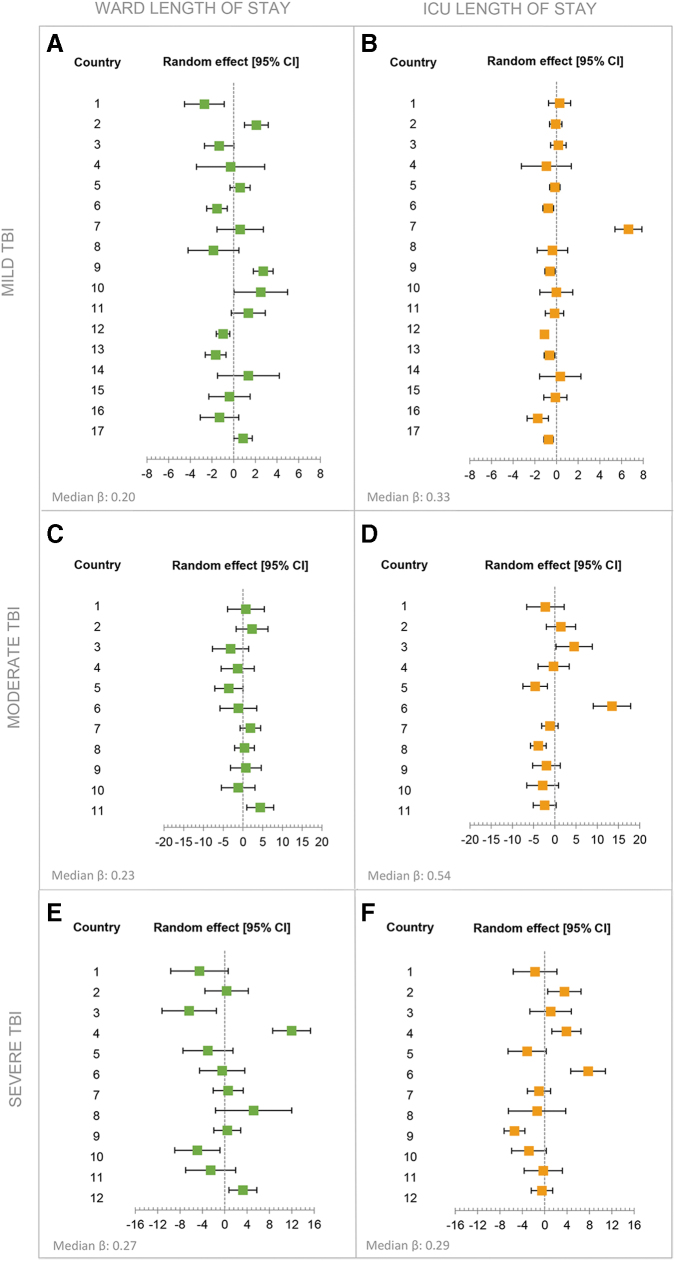
Traumatic brain injury (TBI) is a global public health problem and a leading cause of mortality, morbidity, and disability. The increasing incidence combined with the heterogeneity and complexity of TBI will inevitably place a substantial burden on health systems. These findings emphasize the importance of obtaining accurate and timely insights into healthcare consumption and costs on a multi-national scale. This study aimed to describe intramural healthcare consumption and costs across the full spectrum of TBI in Europe. The Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) core study is a prospective observational study conducted in 18 countries across Europe and in Israel. The baseline Glasgow Coma Scale (GCS) was used to differentiate patients by brain injury severity in mild (GCS 13-15), moderate (GCS 9-12), or severe (GCS ≤8) TBI. We analyzed seven main cost categories: pre-hospital care, hospital admission, surgical interventions, imaging, laboratory, blood products, and rehabilitation. Costs were estimated based on Dutch reference prices and converted to country-specific unit prices using gross domestic product (GDP)-purchasing power parity (PPP) adjustment. Mixed linear regression was used to identify between-country differences in length of stay (LOS), as a parameter of healthcare consumption. Mixed generalized linear models with gamma distribution and log link function quantified associations of patient characteristics with higher total costs. We included 4349 patients, of whom 2854 (66%) had mild, 371 (9%) had moderate, and 962 (22%) had severe TBI. Hospitalization accounted for the largest part of the intramural consumption and costs (60%). In the total study population, the mean LOS was 5.1 days at the intensive care unit (ICU) and 6.3 days at the ward. For mild, moderate, and severe TBI, mean LOS was, respectively, 1.8, 8.9, and 13.5 days at the ICU and 4.5, 10.1, and 10.3 days at the ward. Other large contributors to the total costs were rehabilitation (19%) and intracranial surgeries (8%). Total costs increased with higher age and greater trauma severity (mild; €3,800 [IQR €1,400-14,000], moderate; €37,800 [IQR €14,900-€74,200], severe; €60,400 [IQR €24,400-€112,700]). The adjusted analysis showed that female patients had lower costs than male patients (odds ratio (OR) 0.80 [CI 0.75-1.85]). Increasing TBI severity was associated with higher costs, OR 1.46 (confidence interval [CI] 1.31-1.63) and OR 1.67 [CI 1.52-1.84] for moderate and severe patients, respectively. A worse pre-morbid overall health state, increasing age and more severe systemic trauma, expressed in the Injury Severity Score (ISS), were also significantly associated with higher costs. Intramural costs of TBI are significant and are profoundly driven by hospitalization. Costs increased with trauma severity and age, and male patients incurred higher costs. Reducing LOS could be targeted with advanced care planning, in order to provide cost-effective care.
Keywords: healthcare consumption; healthcare costs; hospital costs; traumatic brain injury;.
Conflict of interest statement
No competing financial interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical