

Effects of prior therapies on outcomes with trifluridine/tipiracil in patients with metastatic gastric/gastroesophageal junction cancer in a randomized phase III trial (TAGS)
- PMID: 37213030
- PMCID: PMC10374776
- DOI: 10.1007/s00432-023-04813-z
Effects of prior therapies on outcomes with trifluridine/tipiracil in patients with metastatic gastric/gastroesophageal junction cancer in a randomized phase III trial (TAGS)
Abstract
Background: In the phase III TAGS trial, trifluridine/tipiracil showed survival benefit versus placebo in patients with metastatic gastric/gastroesophageal junction cancer and ≥ 2 prior chemotherapies. This post hoc exploratory analysis assessed the impact of prior therapy type on outcomes.
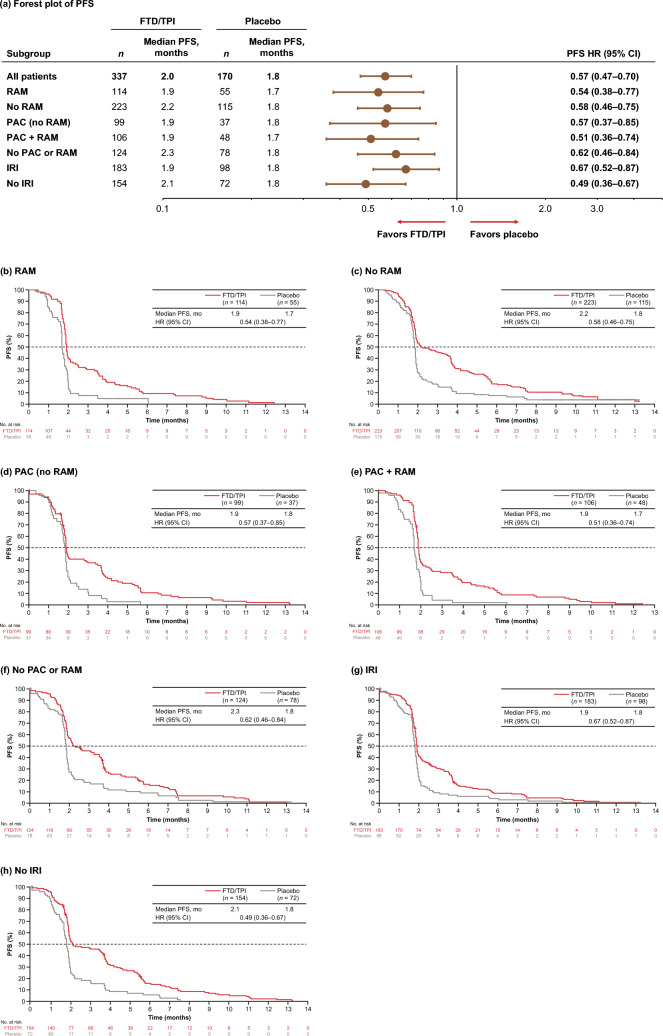
Methods: Based on prior treatment, patients in TAGS (N = 507) were categorized into overlapping subgroups: ramucirumab ± other agents (n = 169), no ramucirumab (n = 338), paclitaxel but no ramucirumab (n = 136), ramucirumab + paclitaxel sequentially or in combination (n = 154), neither paclitaxel nor ramucirumab (n = 202), irinotecan (n = 281), and no irinotecan (n = 226). Overall and progression-free survival, time to Eastern Cooperative Oncology Group performance status (ECOG PS) ≥ 2, and safety were assessed.
Results: Baseline characteristics and prior therapy patterns were generally well balanced between trifluridine/tipiracil and placebo arms across subgroups. Trifluridine/tipiracil was associated with survival benefits versus placebo regardless of prior treatment: across subgroups, median overall survival was 4.6-6.1 versus 3.0-3.8 months (hazard ratios, 0.47-0.88), median progression-free survival was 1.9-2.3 versus 1.7-1.8 months (hazard ratios, 0.49-0.67), and median time to ECOG PS ≥ 2 was 4.0-4.7 versus 1.9-2.5 months (hazard ratios, 0.56-0.88). Among trifluridine/tipiracil-randomized patients, median overall and progression-free survival trended longer in those who had not received ramucirumab, paclitaxel and ramucirumab, or irinotecan (6.0-6.1 and 2.1-2.3 months, respectively) than in those who previously received these agents (4.6-5.7 and 1.9 months). The trifluridine/tipiracil safety profile was consistent across subgroups, with similar overall incidences of grade ≥ 3 adverse events. Minor variations in hematologic toxicities were noted.
Conclusions: In TAGS, third- or later-line trifluridine/tipiracil treatment demonstrated overall and progression-free survival and functioning benefits versus placebo and a consistent safety profile in patients with metastatic gastric/gastroesophageal junction cancer, regardless of prior treatment type.
Clinical trials registration: clinicaltrials.gov NCT02500043.
Keywords: Antineoplastic protocols; Gastric cancer; Gastroesophageal junction cancer; Third- or later-line therapy; Trifluridine tipiracil.
© 2023. The Author(s).
Conflict of interest statement
KS has received institutional research funding from Astellas Pharma, Amgen, Chugai Pharma, Daiichi Sankyo, Eisai, Medi Science, Merck Pharmaceuticals, Ono Pharmaceutical, and Taiho Pharmaceuticals; has served in an advisory capacity for AbbVie Inc, Amgen, Bristol-Myers Squibb, Boehringer Ingelheim, GlaxoSmithKline, Eli Lilly and Company, Janssen, Merck Pharmaceuticals, Novartis, Ono Pharmaceuticals, Pfizer Inc, Taiho Pharmaceuticals, and Takeda Pharmaceuticals; and has received honoraria from Bristol-Myers Squibb and Takeda Pharmaceuticals. BG has received institutional research funding from Boehringer Ingelheim, Glyconex, Helix Biopharma, Hutchison Medipharma, Mirati Therapeutics, NGM Biopharma, Roche/Genentech, Sirnaomics, Taiho Oncology, Toray, and Trishula Therapeutics; consulting fees from BMS, Boston Therapeutics, Exelixis, Foundation Medicine, Ipsen, Pfizer, Roche/Genentech, and Taiho Oncology; and honoraria from BMS, Ipsen, and Taiho Oncology; and has participated in a data safety monitoring board for Roche/Genentech. JT has received consulting fees, honoraria for lectures/presentations and meeting support from Amgen, Astellas, AstraZeneca, BMS, Merck, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, and Servier. RS has received research funding from MSD and Paxman Coolers, has served on the advisory board for Bristol Myers Squibb, Eisai, Bayer, GSK, Merck, MSD, Novartis, and Taiho; has received honoraria for talks from AstraZeneca, BMS, Eli Lilly, DKSH, MSD, Roche, and Taiho; and has received travel support from AstraZeneca, DKSH, Eisai, Roche, and Taiho. MF has received institutional research funding from Amgen, Inc., Bristol Myers Squibb, Genentech, Novartis Oncology, and Verastem; consulting fees from AstraZeneca, Incyte Corporation, PsiOxus, and Taiho Oncology; honoraria from Guardant360, and has participated in an advisory capacity for Amgen, Inc., Bayer Corporation, GlaxoSmithKline, Mirati Therapeutics, Nouscom, and Roche/Genentech. LM is a consultant statistician for Taiho Oncology, Inc. and is paid by Taiho Oncology Inc. KAB is an employee at Taiho Oncology and owns stock of Eli Lilly. MG has served in an advisory capacity for Amgen, Eli Lilly and Company, Merck Pharmaceuticals, Roche, and Servier Pharmaceuticals.
Figures


Similar articles
-
Trastuzumab Deruxtecan or Ramucirumab plus Paclitaxel in Gastric Cancer.N Engl J Med. 2025 Jul 24;393(4):336-348. doi: 10.1056/NEJMoa2503119. Epub 2025 May 31. N Engl J Med. 2025. PMID: 40454632 Clinical Trial.
-
Real-World Effectiveness and Safety of Ramucirumab as a Second-Line Treatment for Patients with Unresectable Advanced or Metastatic Gastric/Gastroesophageal Junction Adenocarcinoma in Japan and South Korea: A Systematic Literature Review.Adv Ther. 2024 Jun;41(6):2112-2132. doi: 10.1007/s12325-024-02838-5. Epub 2024 Apr 15. Adv Ther. 2024. PMID: 38619719 Free PMC article.
-
Trifluridine-Tipiracil and Bevacizumab in Refractory Metastatic Colorectal Cancer.N Engl J Med. 2023 May 4;388(18):1657-1667. doi: 10.1056/NEJMoa2214963. N Engl J Med. 2023. PMID: 37133585 Clinical Trial.
-
Targeted therapy combined with immunotherapy vs trifluridine/tipiracil with bevacizumab as late-line therapy in metastatic colorectal cancer.World J Gastroenterol. 2025 Aug 7;31(29):109947. doi: 10.3748/wjg.v31.i29.109947. World J Gastroenterol. 2025. PMID: 40809924 Free PMC article.
-
Palliative chemotherapy and targeted therapies for esophageal and gastroesophageal junction cancer.Cochrane Database Syst Rev. 2017 Nov 28;11(11):CD004063. doi: 10.1002/14651858.CD004063.pub4. Cochrane Database Syst Rev. 2017. PMID: 29182797 Free PMC article.
References
-
- Chrom P, Stec R, Szczylik C (2015) Second-line treatment of advanced gastric cancer: current options and future perspectives. Anticancer Res 35:4575–4583 - PubMed
-
- Depetris I, Marino D, Bonzano A, Cagnazzo C, Filippi R, Aglietta M et al (2018) Fluoropyrimidine-induced cardiotoxicity. Crit Rev Oncol Hematol 124:1–10 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
