

Efficacy and Safety of Oral Small Molecule Glucagon-Like Peptide 1 Receptor Agonist Danuglipron for Glycemic Control Among Patients With Type 2 Diabetes: A Randomized Clinical Trial
- PMID: 37213102
- PMCID: PMC10203889
- DOI: 10.1001/jamanetworkopen.2023.14493
Efficacy and Safety of Oral Small Molecule Glucagon-Like Peptide 1 Receptor Agonist Danuglipron for Glycemic Control Among Patients With Type 2 Diabetes: A Randomized Clinical Trial
Abstract
Importance: Currently available glucagon-like peptide 1 receptor (GLP-1R) agonists for treating type 2 diabetes (T2D) are peptide agonists that require subcutaneous administration or strict fasting requirements before and after oral administration.
Objective: To investigate the efficacy, safety, and tolerability of multiple dose levels of the novel, oral, small molecule GLP-1R agonist danuglipron over 16 weeks.
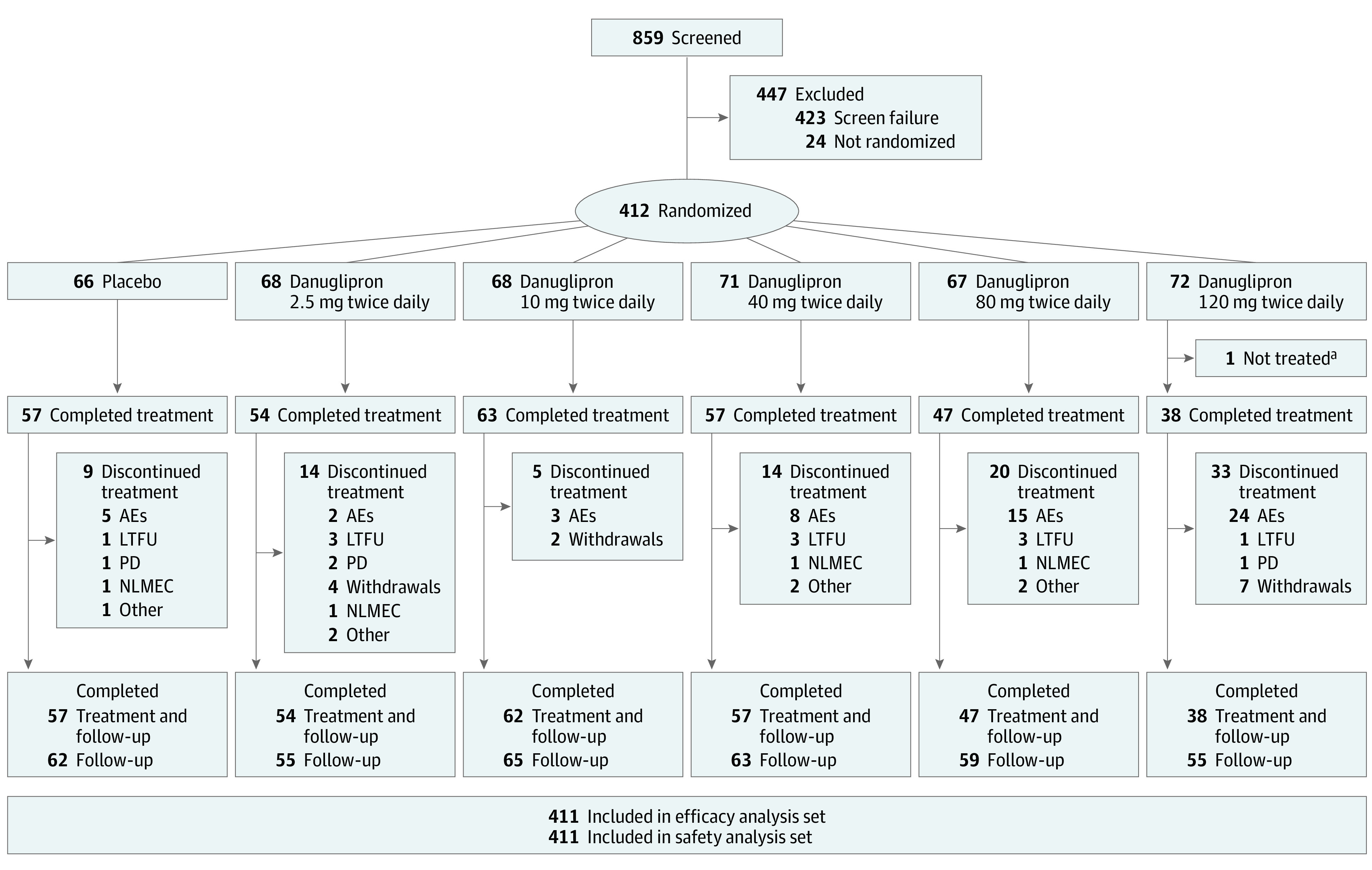
Design, setting, and participants: A phase 2b, double-blind, placebo-controlled, parallel-group, 6-group randomized clinical trial with 16-week double-blind treatment period and 4-week follow-up was conducted from July 7, 2020, to July 7, 2021. Adults with T2D inadequately controlled by diet and exercise, with or without metformin treatment, were enrolled from 97 clinical research sites in 8 countries or regions.
Interventions: Participants received placebo or danuglipron, 2.5, 10, 40, 80, or 120 mg, all orally administered twice daily with food for 16 weeks. Weekly dose escalation steps were incorporated to achieve danuglipron doses of 40 mg or more twice daily.
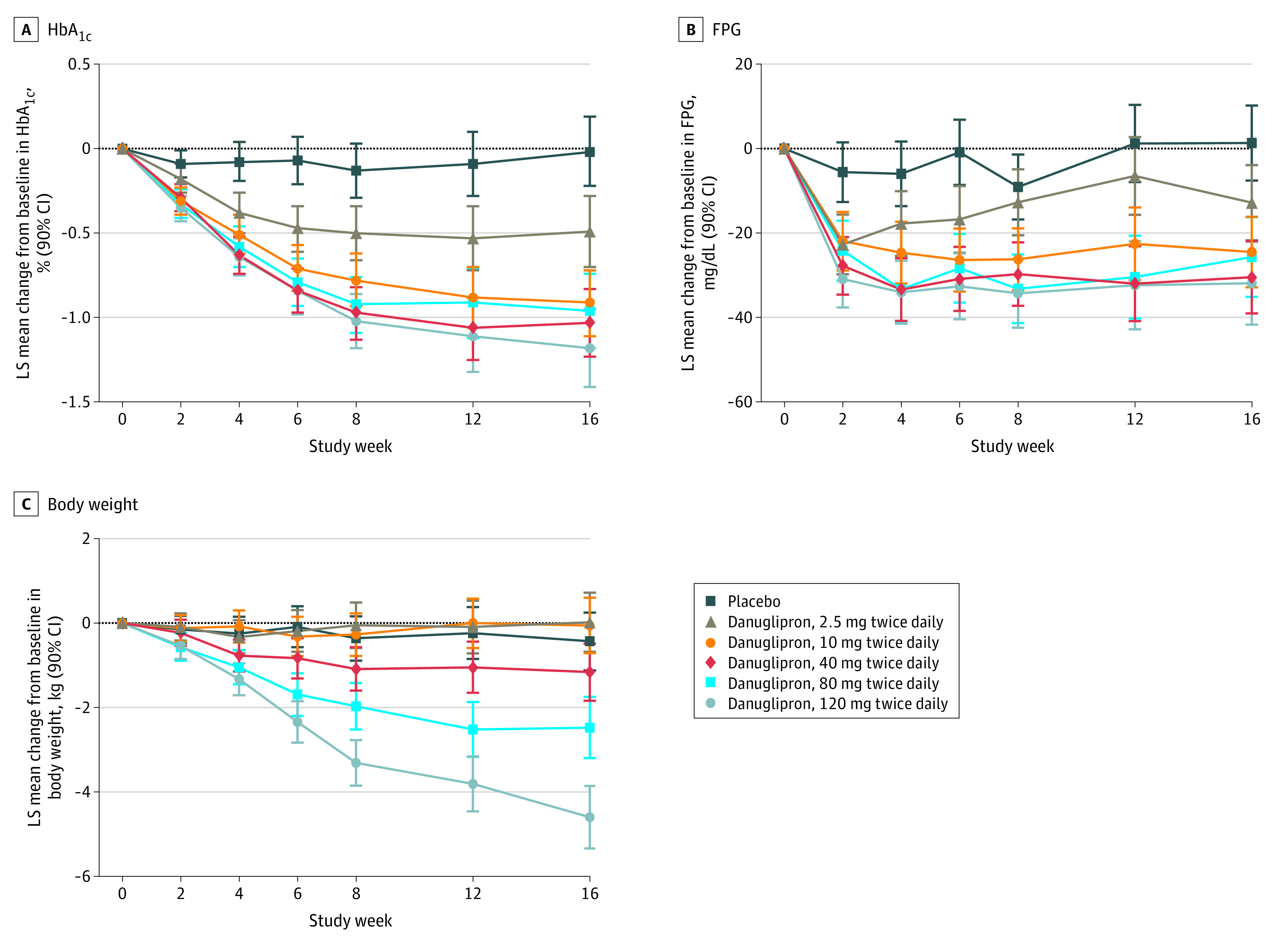
Main outcomes and measures: Change from baseline in glycated hemoglobin (HbA1c, primary end point), fasting plasma glucose (FPG), and body weight were assessed at week 16. Safety was monitored throughout the study period, including a 4-week follow-up period.
Results: Of 411 participants randomized and treated (mean [SD] age, 58.6 [9.3] years; 209 [51%] male), 316 (77%) completed treatment. For all danuglipron doses, HbA1c and FPG were statistically significantly reduced at week 16 vs placebo, with HbA1c reductions up to a least squares mean difference vs placebo of -1.16% (90% CI, -1.47% to -0.86%) for the 120-mg twice daily group and FPG reductions up to a least squares mean difference vs placebo of -33.24 mg/dL (90% CI, -45.63 to -20.84 mg/dL). Body weight was statistically significantly reduced at week 16 compared with placebo in the 80-mg twice daily and 120-mg twice daily groups only, with a least squares mean difference vs placebo of -2.04 kg (90% CI, -3.01 to -1.07 kg) for the 80-mg twice daily group and -4.17 kg (90% CI, -5.15 to -3.18 kg) for the 120-mg twice daily group. The most commonly reported adverse events were nausea, diarrhea, and vomiting.
Conclusions and relevance: In adults with T2D, danuglipron reduced HbA1c, FPG, and body weight at week 16 compared with placebo, with a tolerability profile consistent with the mechanism of action.
Trial registration: ClinicalTrials.gov Identifier: NCT03985293.
Conflict of interest statement
Figures
References
-
- Buse JB, Wexler DJ, Tsapas A, et al. . 2019 update to: management of hyperglycemia in type 2 diabetes, 2018: a consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020;43(2):487-493. doi:10.2337/dci19-0066 - DOI - PMC - PubMed
-
- Sikirica MV, Martin AA, Wood R, Leith A, Piercy J, Higgins V. Reasons for discontinuation of GLP1 receptor agonists: data from a real-world cross-sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;10:403-412. doi:10.2147/DMSO.S141235 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
