

Comparative Effects of Glucose-Lowering Medications on Kidney Outcomes in Type 2 Diabetes: The GRADE Randomized Clinical Trial
- PMID: 37213109
- PMCID: PMC10203973
- DOI: 10.1001/jamainternmed.2023.1487
Comparative Effects of Glucose-Lowering Medications on Kidney Outcomes in Type 2 Diabetes: The GRADE Randomized Clinical Trial
Abstract
Importance: Type 2 diabetes (T2D) is the leading cause of kidney disease in the US. It is not known whether glucose-lowering medications differentially affect kidney function.
Objective: To evaluate kidney outcomes in the Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness (GRADE) trial comparing 4 classes of glucose-lowering medications added to metformin for glycemic management in individuals with T2D.
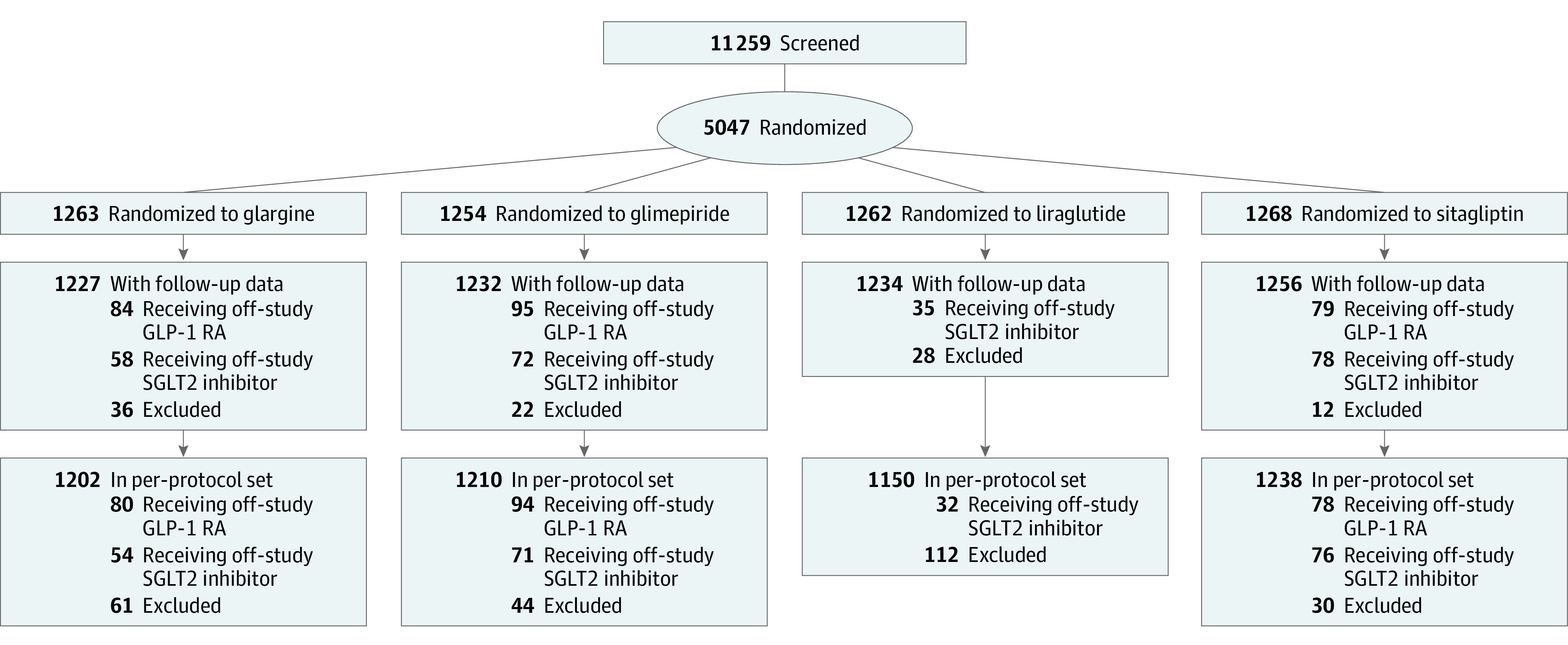
Design, setting, and participants: A randomized clinical trial was conducted at 36 sites across the US. Participants included adults with T2D for less than 10 years, a hemoglobin A1c level between 6.8% and 8.5%, and estimated glomerular filtration rate (eGFR) greater than or equal to 60 mL/min/1.73 m2 who were receiving metformin treatment. A total of 5047 participants were enrolled between July 8, 2013, and August 11, 2017, and followed up for a mean of 5.0 years (range, 0-7.6 years). Data were analyzed from February 21, 2022, to March 27, 2023.
Interventions: Addition of insulin glargine, glimepiride, liraglutide, or sitagliptin to metformin, with the medication combination continued until the HbA1c was greater than 7.5%; thereafter, insulin was added to maintain glycemic control.
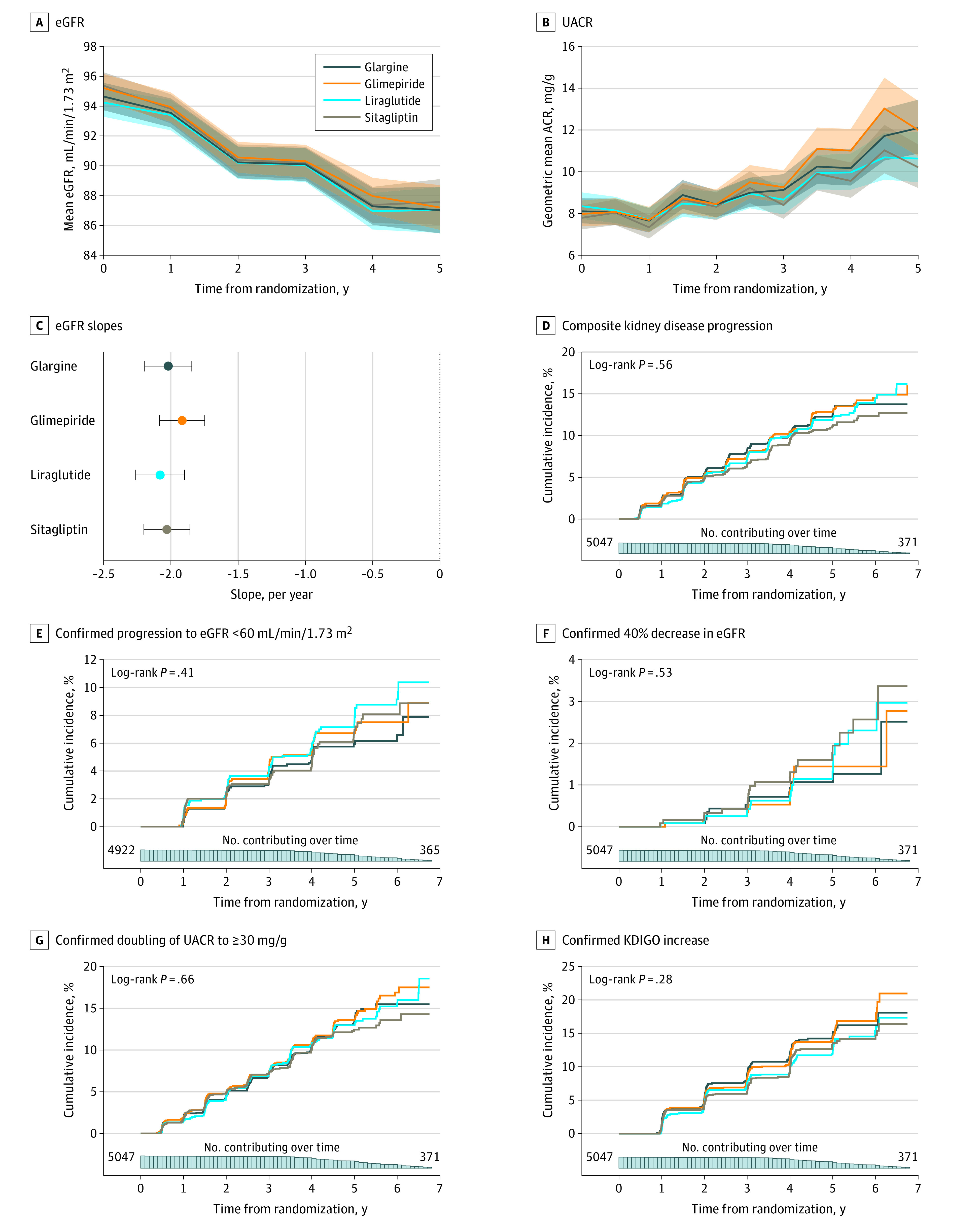
Main outcomes and measures: Chronic eGFR slope (change in eGFR between year 1 and trial end) and a composite kidney disease progression outcome (albuminuria, dialysis, transplant, or death due to kidney disease). Secondary outcomes included incident eGFR less than 60 mL/min/1.73 m2, 40% decrease in eGFR to less than 60 mL/min/1.73 m2, doubling of urine albumin-to-creatinine ratio (UACR) to 30 mg/g or greater, and progression of Kidney Disease Improving Global Outcomes stage. Analyses were intention-to-treat.
Results: Of the 5047 participants, 3210 (63.6%) were men. Baseline characteristics were mean (SD) age 57.2 (10.0) years; HbA1c 7.5% (0.5%); diabetes duration, 4.2 (2.7) years; body mass index, 34.3 (6.8); blood pressure 128.3/77.3 (14.7/9.9) mm Hg; eGFR 94.9 (16.8) mL/min/1.73 m2; and median UACR, 6.4 (IQR 3.1-16.9) mg/g; 2933 (58.1%) were treated with renin-angiotensin-aldosterone inhibitors. Mean chronic eGFR slope was -2.03 (95% CI, -2.20 to -1.86) mL/min/1.73 m2 per year for patients receiving sitagliptin; glimepiride, -1.92 (95% CI, -2.08 to -1.75) mL/min/1.73 m2 per year; liraglutide, -2.08 (95% CI, -2.26 to -1.90) mL/min/1.73 m2 per year; and insulin glargine, -2.02 (95% CI, -2.19 to -1.84) mL/min/1.73 m2 per year (P = .61). Mean composite kidney disease progression occurred in 135 (10.6%) patients receiving sitagliptin; glimepiride, 155 (12.4%); liraglutide, 152 (12.0%); and insulin glargine, 150 (11.9%) (P = .56). Most of the composite outcome was attributable to albuminuria progression (98.4%). There were no significant differences by treatment assignment in secondary outcomes. There were no adverse kidney events attributable to medication assignment.
Conclusions and relevance: In this randomized clinical trial, among people with T2D and predominantly free of kidney disease at baseline, no significant differences in kidney outcomes were observed during 5 years of follow-up when a dipeptidyl peptidase 4 inhibitor, sulfonylurea, glucagonlike peptide 1 receptor agonist, or basal insulin was added to metformin for glycemic control.
Trial registration: ClinicalTrials.gov Identifier: NCT01794143.
Conflict of interest statement
Figures
References
-
- Coca SG, Ismail-Beigi F, Haq N, Krumholz HM, Parikh CR. Role of intensive glucose control in development of renal end points in type 2 diabetes mellitus: systematic review and meta-analysis intensive glucose control in type 2 diabetes. Arch Intern Med. 2012;172(10):761-769. doi:10.1001/archinternmed.2011.2230 - DOI - PMC - PubMed
-
- Zoungas S, Arima H, Gerstein HC, et al. ; Collaborators on Trials of Lowering Glucose (CONTROL) group . Effects of intensive glucose control on microvascular outcomes in patients with type 2 diabetes: a meta-analysis of individual participant data from randomised controlled trials. Lancet Diabetes Endocrinol. 2017;5(6):431-437. doi:10.1016/S2213-8587(17)30104-3 - DOI - PubMed
-
- DCCT/EDIC research group . Effect of intensive diabetes treatment on albuminuria in type 1 diabetes: long-term follow-up of the Diabetes Control and Complications Trial and Epidemiology of Diabetes Interventions and Complications study. Lancet Diabetes Endocrinol. 2014;2(10):793-800. doi:10.1016/S2213-8587(14)70155-X - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR002537/TR/NCATS NIH HHS/United States
- UL1 TR000170/TR/NCATS NIH HHS/United States
- U34 DK088043/DK/NIDDK NIH HHS/United States
- P30 DK072476/DK/NIDDK NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- U01 DK098246/DK/NIDDK NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- UL1 TR002529/TR/NCATS NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
- P30 DK020541/DK/NIDDK NIH HHS/United States
- P30 DK092926/DK/NIDDK NIH HHS/United States
- P30 DK124723/DK/NIDDK NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- U01 DK119083/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- P30 DK020579/DK/NIDDK NIH HHS/United States
- P30 DK020572/DK/NIDDK NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
