

This is a preprint.
Delineating clinical and developmental outcomes in STXBP1-related disorders
- PMID: 37215006
- PMCID: PMC10197795
- DOI: 10.1101/2023.05.10.23289776
Delineating clinical and developmental outcomes in STXBP1-related disorders
Update in
-
Delineating clinical and developmental outcomes in STXBP1-related disorders.Brain. 2023 Dec 1;146(12):5182-5197. doi: 10.1093/brain/awad287. Brain. 2023. PMID: 38015929 Free PMC article.
Abstract
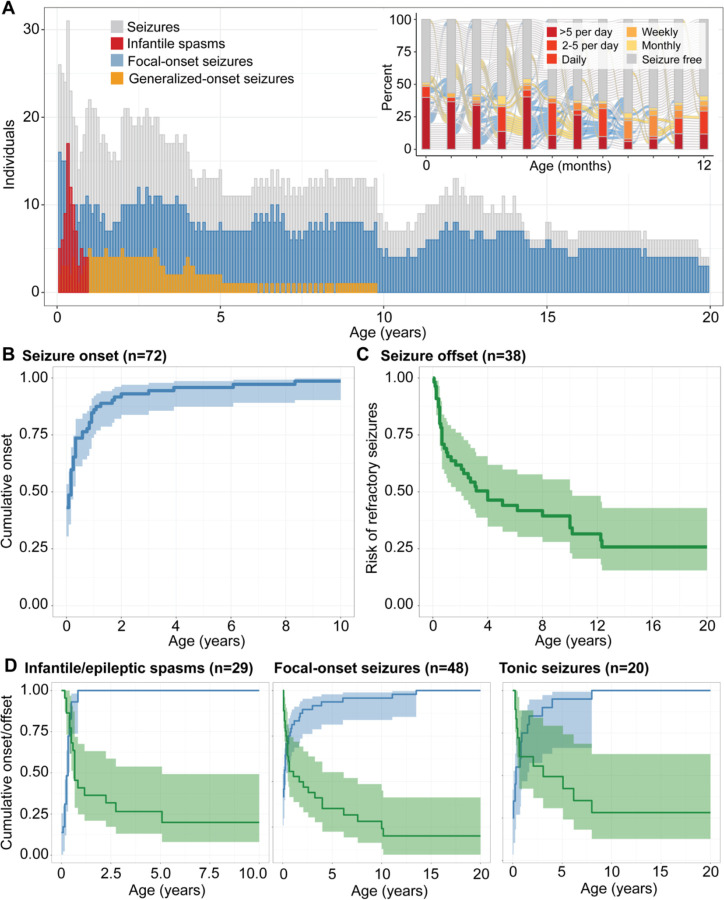
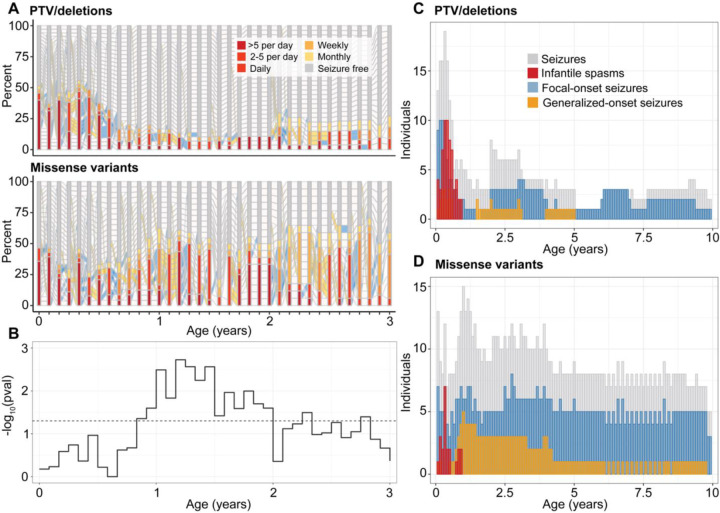
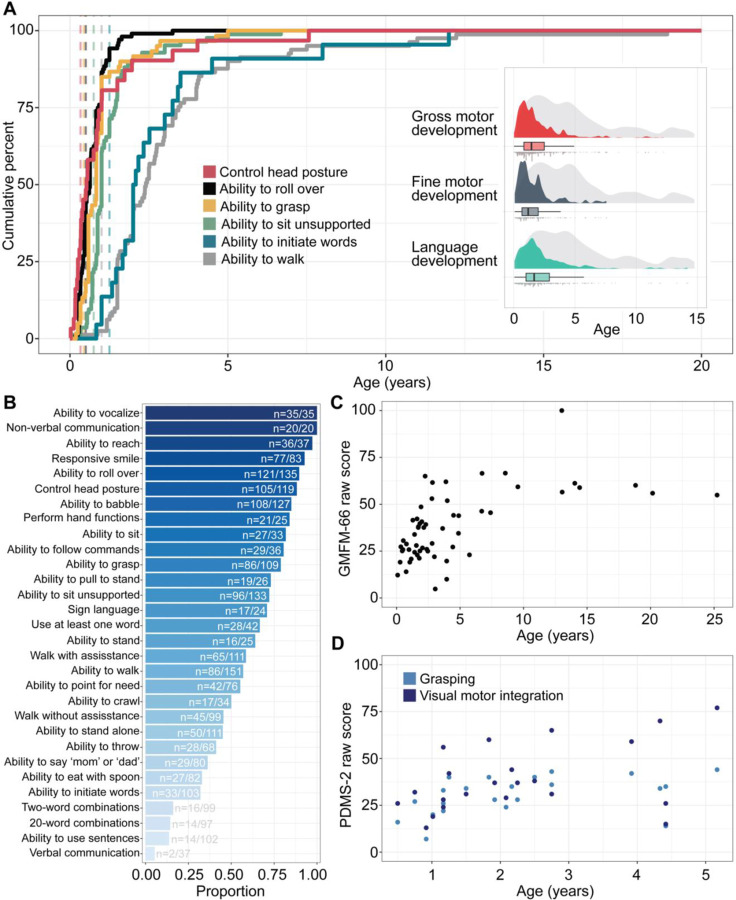
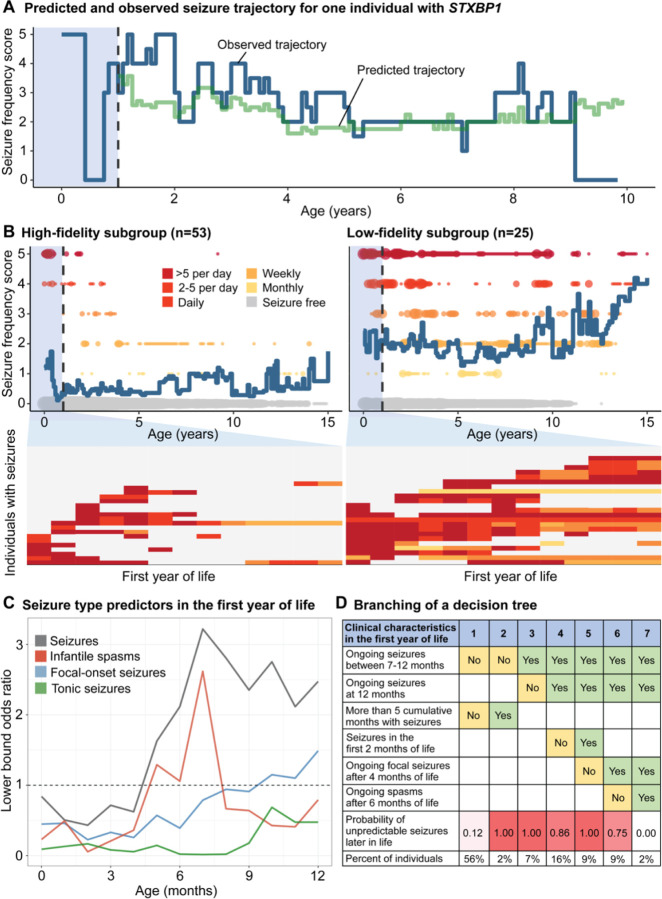
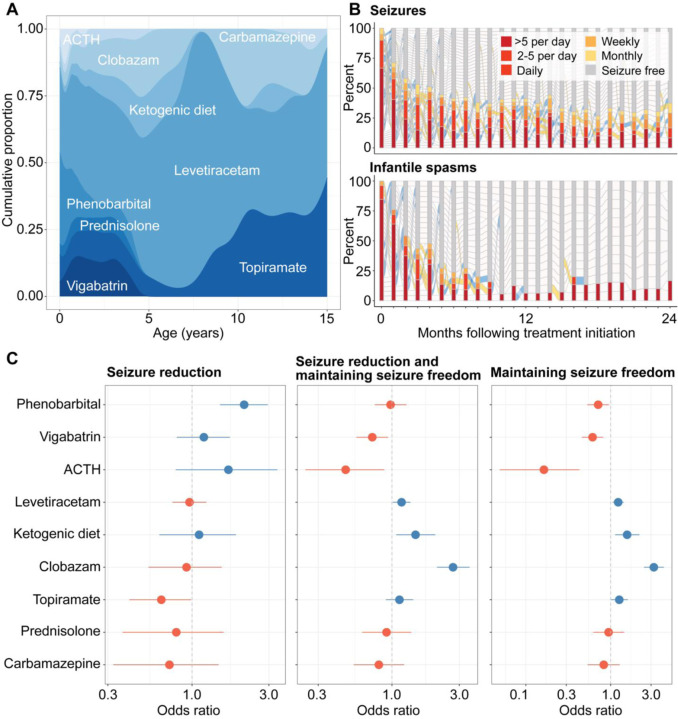
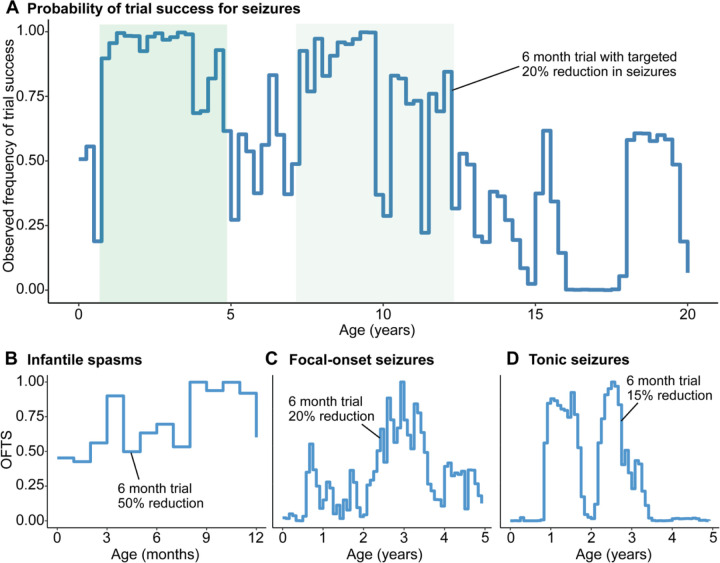
STXBP1-related disorders are among the most common genetic epilepsies and neurodevelopmental disorders. However, the longitudinal epilepsy course and developmental endpoints have not yet been described in detail, which is a critical prerequisite for clinical trial readiness. Here, we assessed 1,281 cumulative patient-years of seizure and developmental histories in 162 individuals with STXBP1-related disorders and established a natural history framework. STXBP1-related disorders are characterized by a dynamic pattern of seizures in the first year of life and high variability in neurodevelopmental trajectories in early childhood. Epilepsy onset differed across seizure types, with 90% cumulative onset for infantile spasms by 6 months and focal-onset seizures by 27 months of life. Epilepsy histories diverged between variant subgroups in the first 2 years of life, when individuals with protein-truncating variants and deletions in STXBP1 (n=39) were more likely to have infantile spasms between 5 and 6 months followed by seizure remission, while individuals with missense variants (n=30) had an increased risk for focal seizures and ongoing seizures after the first year. Developmental outcomes were mapped using milestone acquisition data in addition to standardized assessments including the Gross Motor Function Measure-66 Item Set and the Grasping and Visual-Motor Integration subsets of the Peabody Developmental Motor Scales. Quantification of endpoints revealed high variability during the first five years of life, with emerging stratification between clinical subgroups, most prominently between individuals with and without infantile spasms. We found that individuals with neonatal seizures or early infantile seizures followed by seizure offset by 12 months of life had more predictable seizure trajectories in early to late childhood than compared to individuals with more severe seizure presentations, including individuals with refractory epilepsy throughout the first year. Characterization of anti-seizure medication response revealed age-dependent response over time, with phenobarbital, levetiracetam, topiramate, and adrenocorticotropic hormone effective in reducing seizures in the first year of life, while clobazam and the ketogenic diet were effective in long-term seizure management. Virtual clinical trials using seizure frequency as the primary outcome resulted in wide range of trial success probabilities across the age span, with the highest probability in early childhood between 1 year and 3.5 years. In summary, we delineated epilepsy and developmental trajectories in STXBP1-related disorders using standardized measures, providing a foundation to interpret future therapeutic strategies and inform rational trial design.
Keywords: STXBP1; developmental and epileptic encephalopathy; genetics; natural history study; outcome measures.
Conflict of interest statement
Authors conflicts of interest: All authors declare no conflict of interest. Competing interests All other authors do not declare any competing interests.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources