

Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
- PMID: 37215744
- PMCID: PMC10198174
- DOI: 10.2147/COPD.S397361
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Abstract
Background: Pulmonary rehabilitation (PR) effectively improves symptoms and exercise ability in patients with stable chronic obstructive pulmonary disease (COPD). However, the effectiveness and timing of early PR on hospitalized patients with acute exacerbation of COPD (AECOPD) is still debated.
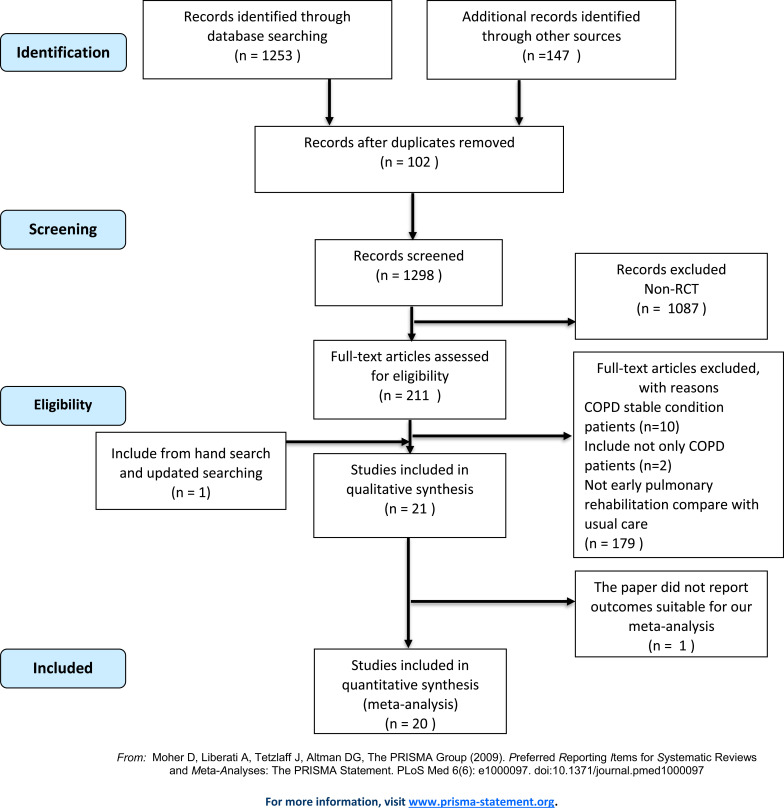
Methods: This study conducted a meta-analysis to compare the outcome benefits between early PR and usual care for patient hospitalized due to AECOPD. A systematic search was performed for retrieving randomized control trials (RCTs) from the PubMed, Embase, and Cochrane library until November 2021. RCTs reporting early PR for AECOPD with hospitalization, either during admission or within four weeks of discharge, were enrolled for systematic review and meta-analysis.
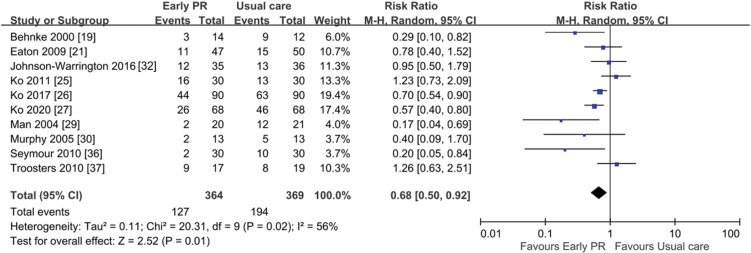
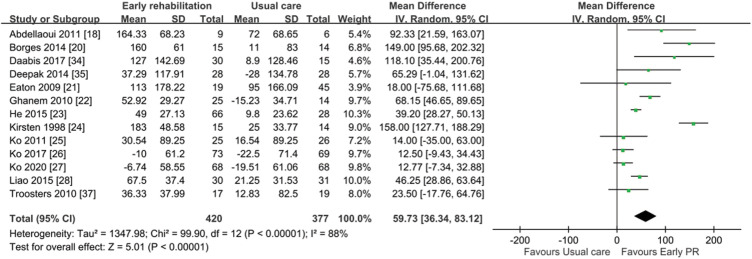
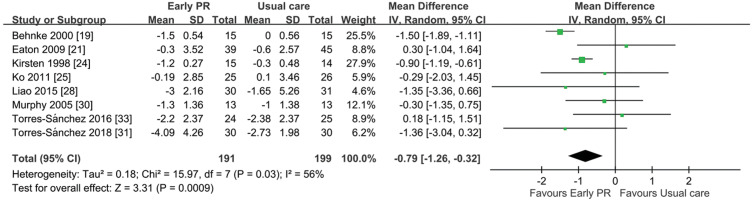
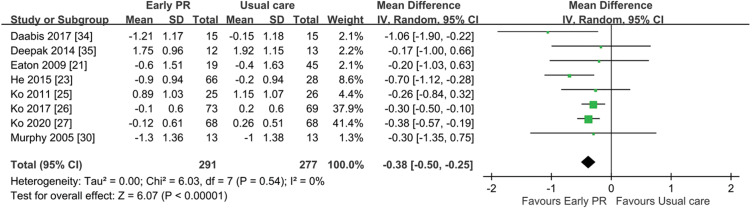
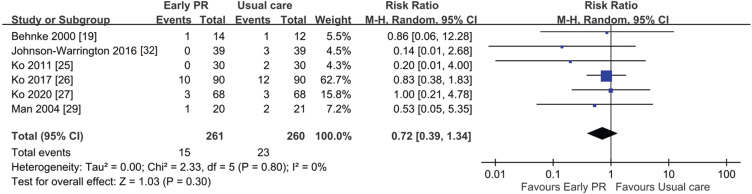
Results: Twenty RCTs (1274 participants) were included. Early PR showed significantly improved readmission rate (ten trials, risk ratio 0.68, 95% confidence interval (CI) 0.50-0.92), 6-minute walking distance (6MWD, twelve trials, MD 59.73, 95% CI 36.34-83.12), St George's Respiratory Questionnaire score (eight trials, MD -10.65, 95% CI -14.78 to -6.52), Borg score (eight trials, MD -0.79, 95% CI -1.26 to -0.32), and modified Medical Research Council dyspnea scale (eight trials, MD -0.38, 95% CI -0.5 to -0.25). However, the trend of mortality (six trials, risk ratio 0.72, 95% CI 0.39-1.34) benefit was not significant. The subgroup analysis showed non-significant trends of better effect in early PR during admission than those after discharge for outcomes of 6MWD, quality of life, and dyspnea. However, non-significant trends of less benefits on mortality and readmission rate were found in early PR during the admission.
Conclusion: Overall, early PR is beneficial for AECOPD with hospitalization, and there was no significant outcome difference between PR initiated during admission or within 4 weeks of discharge.
Keywords: chronic obstructive pulmonary disease; exacerbation; hospitalization; pulmonary rehabilitation.
© 2023 Lu et al.
Conflict of interest statement
Dr Pei-Chin Lin reports grants from Kaohsiung Veterans General Hospital and the Ministry of Science and Technology of Taiwan. The other authors report no conflicts of interest in this work.
Figures

References
-
- Global Initiative for Chronic Obstructive Lung Disease. 2020 Global strategy for prevention, diagnosis and management of COPD (2020 report). Available from: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-0.... Accessed September 19, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
