

Do Dosiomic Features Extracted From Planned 3-Dimensional Dose Distribution Improve Biochemical Failure-Free Survival Prediction: an Analysis Based on a Large Multi-Institutional Data Set
- PMID: 37216005
- PMCID: PMC10195848
- DOI: 10.1016/j.adro.2023.101227
Do Dosiomic Features Extracted From Planned 3-Dimensional Dose Distribution Improve Biochemical Failure-Free Survival Prediction: an Analysis Based on a Large Multi-Institutional Data Set
Abstract
Purpose: The objective of this work was to investigate whether including additional dosiomic features can improve biochemical failure-free survival prediction compared with models with clinical features only or with clinical features as well as equivalent uniform dose and tumor control probability.
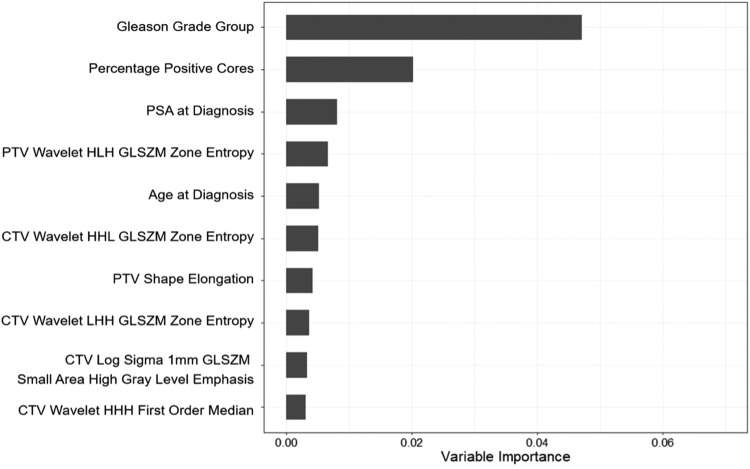
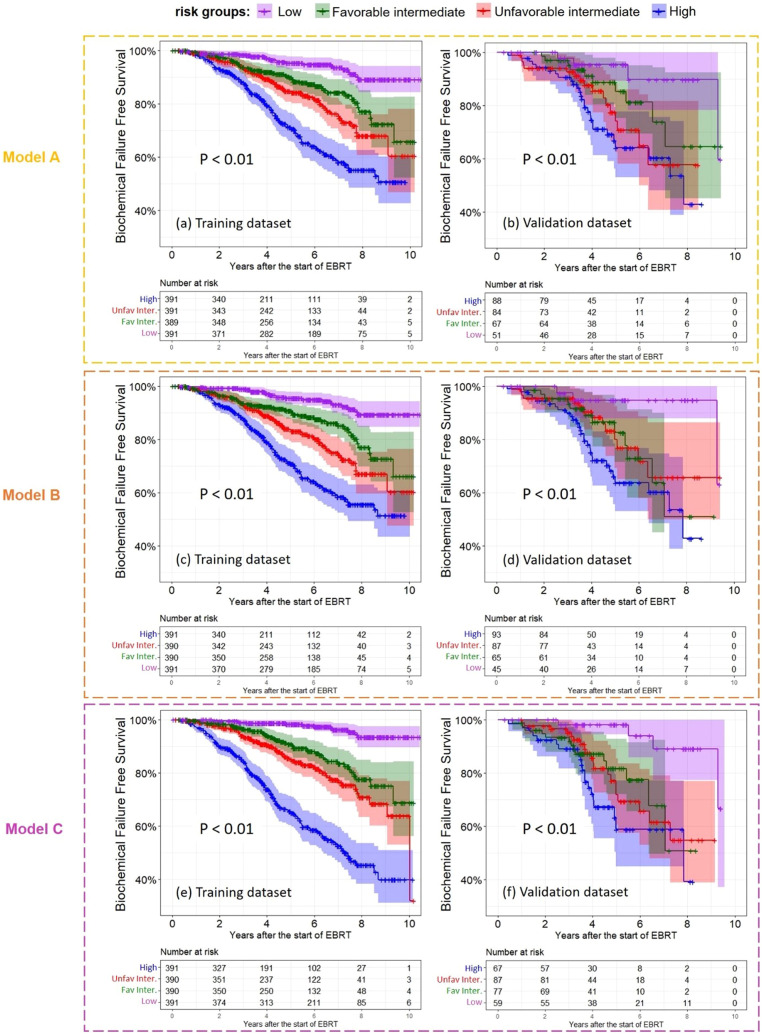
Methods and materials: This retrospective study included 1852 patients who received diagnoses of localized prostate cancer between 2010 and 2016 and were treated with curative external beam radiation therapy in Albert, Canada. A total of 1562 patients from 2 centers were used for developing 3 random survival forest models: Model A included only 5 clinical features; Model B included 5 clinical features, equivalent uniform dose, and tumor control probability; and Model C considered 5 clinical features and 2074 dosiomic features derived from the planned dose distribution of the clinical target volume and planning target volume with further feature selection to determine prognostic features. No feature selection was performed for models A and B. Two hundred ninety patients from another 2 centers were used for independent validation. Individual model-based risk stratification was examined, and the log-rank tests were performed to test statistically significant differences between the risk groups. The 3 models' performances were evaluated using Harrell's concordance index (C-index) and compared using one-way repeated-measures analysis of variance with post hoc paired t test.
Results: Model C selected 6 dosiomic features and 4 clinical features to be prognostic. There were statistically significant differences between the 4 risk groups for both training and validation data sets. The C-index for the out-of-bag samples of the training data set was 0.650, 0.648, and 0.669 for models A, B, and C, respectively. The C-index for the validation data set for models A, B, and C was 0.653, 0.648, and 0.662, respectively. Although gains were modest, Model C was statistically significantly better than models A and B.
Conclusions: Dosiomics contain information beyond common dose-volume histogram metrics from planned dose distributions. Incorporation of prognostic dosiomic features in biochemical failure-free survival outcome models can lead to statistically significant although modest improvement in performance.
© 2023 The Authors.
Figures


References
-
- Phillips R, Hazell S, Song DY. In: Campbell Walsh Wein Urology. 12th ed. Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, editors. Elsevier; Philadelphia, PA: 2021. Radiation therapy for prostate cancer; pp. 3587–3615.
-
- Grimm P, Billiet I, Bostwick D, et al. Comparative analysis of prostate-specific antigen free survival outcomes for patients with low, intermediate and high risk prostate cancer treatment by radical therapy. Results from the Prostate Cancer Results Study Group. BJU Int. 2012;109(suppl 1):22–29. - PubMed
-
- Goy BW, Burchette R, Soper MS, Chang T, Cosmatos HA. Ten-year treatment outcomes of radical prostatectomy vs external beam radiation therapy vs brachytherapy for 1503 patients with intermediate-risk prostate cancer. Urology. 2020;136:180–189. - PubMed
LinkOut - more resources
Full Text Sources
