

Genome-wide mRNA profiling in urinary extracellular vesicles reveals stress gene signature for diabetic kidney disease
- PMID: 37216114
- PMCID: PMC10193229
- DOI: 10.1016/j.isci.2023.106686
Genome-wide mRNA profiling in urinary extracellular vesicles reveals stress gene signature for diabetic kidney disease
Abstract
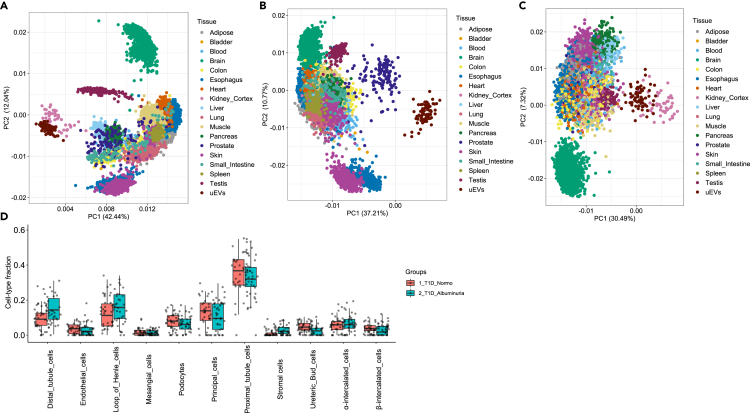
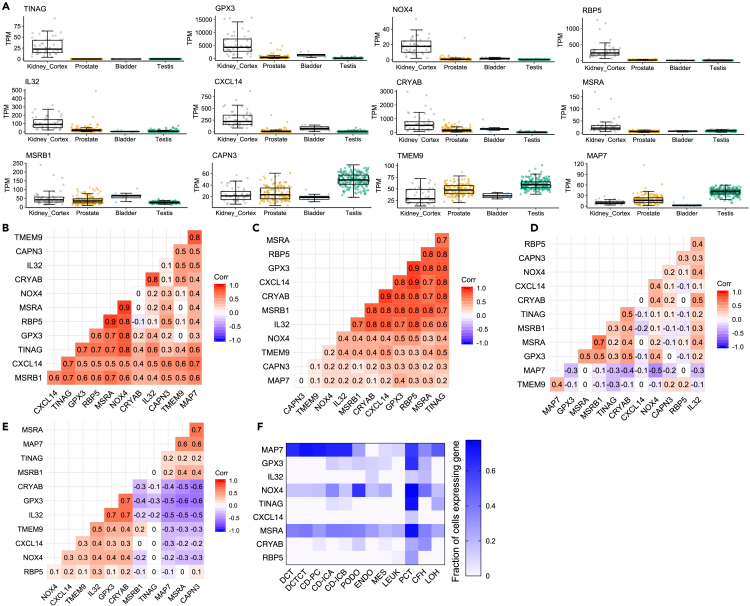
Urinary extracellular vesicles (uEV) are a largely unexplored source of kidney-derived mRNAs with potential to serve as a liquid kidney biopsy. We assessed ∼200 uEV mRNA samples from clinical studies by genome-wide sequencing to discover mechanisms and candidate biomarkers of diabetic kidney disease (DKD) in Type 1 diabetes (T1D) with replication in Type 1 and 2 diabetes. Sequencing reproducibly showed >10,000 mRNAs with similarity to kidney transcriptome. T1D DKD groups showed 13 upregulated genes prevalently expressed in proximal tubules, correlated with hyperglycemia and involved in cellular/oxidative stress homeostasis. We used six of them (GPX3, NOX4, MSRB, MSRA, HRSP12, and CRYAB) to construct a transcriptional "stress score" that reflected long-term decline of kidney function and could even identify normoalbuminuric individuals showing early decline. We thus provide workflow and web resource for studying uEV transcriptomes in clinical urine samples and stress-linked DKD markers as potential early non-invasive biomarkers or drug targets.
Keywords: Biopsy sample; Clinical finding; Disease; Medicine; Specimen.
© 2023 The Author(s).
Conflict of interest statement
L.G. has received research funding from Pfizer Inc, Regeneron Pharmaceuticals, Eli Lilly, and AstraZeneca. P-H.G. has received research grants from Eli Lilly and Roche; is an advisory board member for AbbVie, AstraZeneca, Boehringer Ingelheim, Cebix, Eli Lilly, Jansen, MSD, Novartis, Novo Nordisk, and Sanofi; and has received lecture fees from Boehringer Ingelheim, Eli Lilly, Elo Water, Genzyme, MSD, Novartis, Novo Nordisk, and Sanofi. The funding sources were not involved in the design or conduct of the study.
Figures






References
-
- Gross J.L., de Azevedo M.J., Silveiro S.P., Canani L.H., Caramori M.L., Zelmanovitz T. Diabetic nephropathy: diagnosis, prevention, and treatment. Diabetes Care. 2005;28:164–176. - PubMed
-
- Selby N.M., Taal M.W. An updated overview of diabetic nephropathy: diagnosis, prognosis, treatment goals and latest guidelines. Diabetes Obes. Metab. 2020;22:3–15. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
