

Telemonitoring for heart failure: a meta-analysis
- PMID: 37216272
- PMCID: PMC10424885
- DOI: 10.1093/eurheartj/ehad280
Telemonitoring for heart failure: a meta-analysis
Erratum in
-
Correction to: Telemonitoring for heart failure: a meta-analysis.Eur Heart J. 2025 Oct 14;46(39):3935-3937. doi: 10.1093/eurheartj/ehaf509. Eur Heart J. 2025. PMID: 40838796 Free PMC article. No abstract available.
Abstract
Aims: Telemonitoring modalities in heart failure (HF) have been proposed as being essential for future organization and transition of HF care, however, efficacy has not been proven. A comprehensive meta-analysis of studies on home telemonitoring systems (hTMS) in HF and the effect on clinical outcomes are provided.
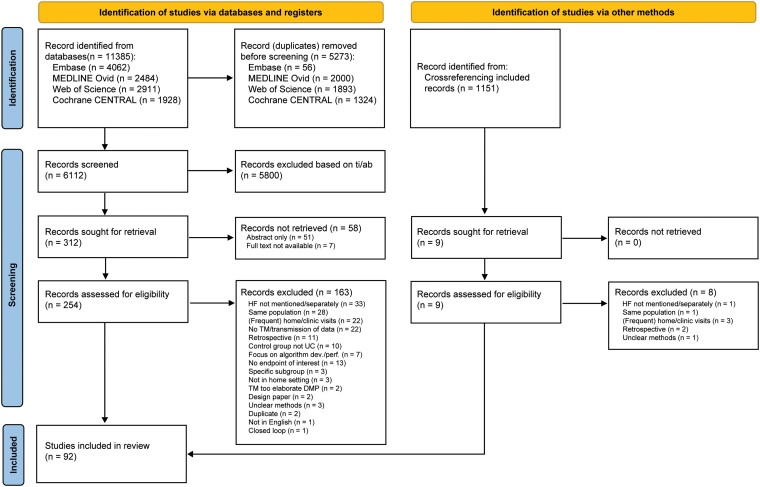
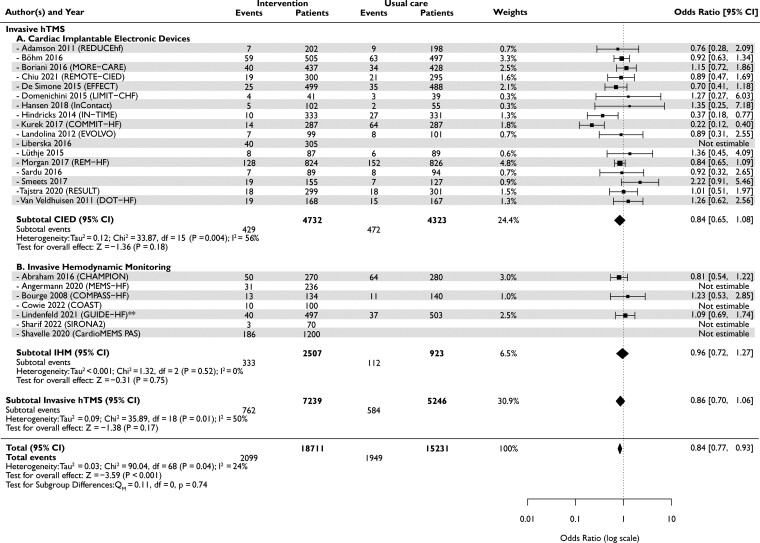
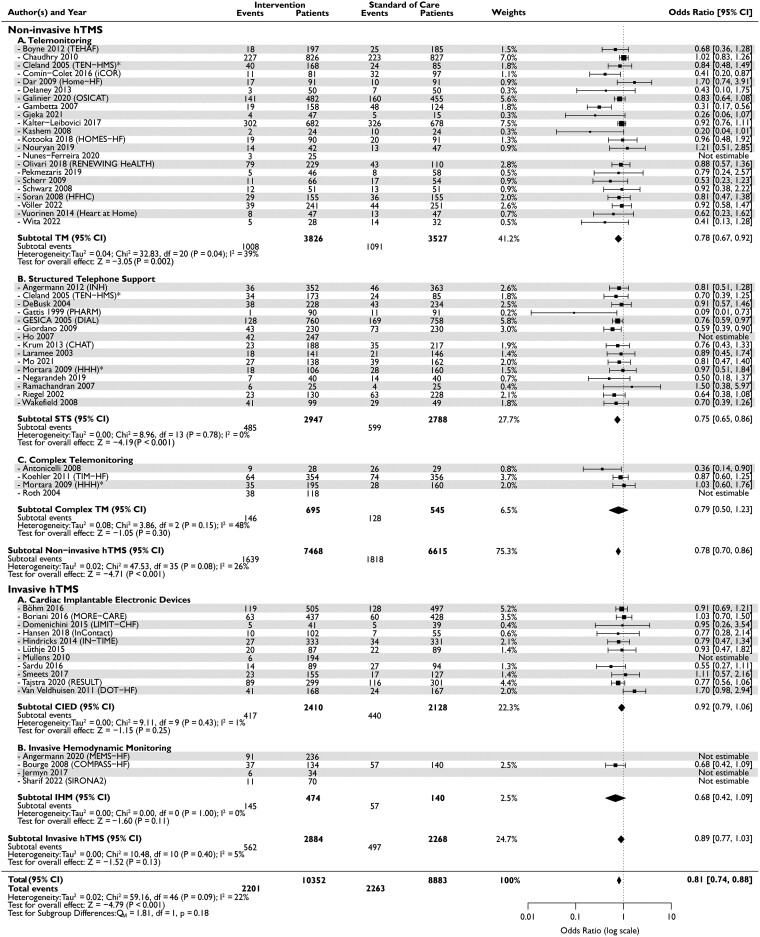
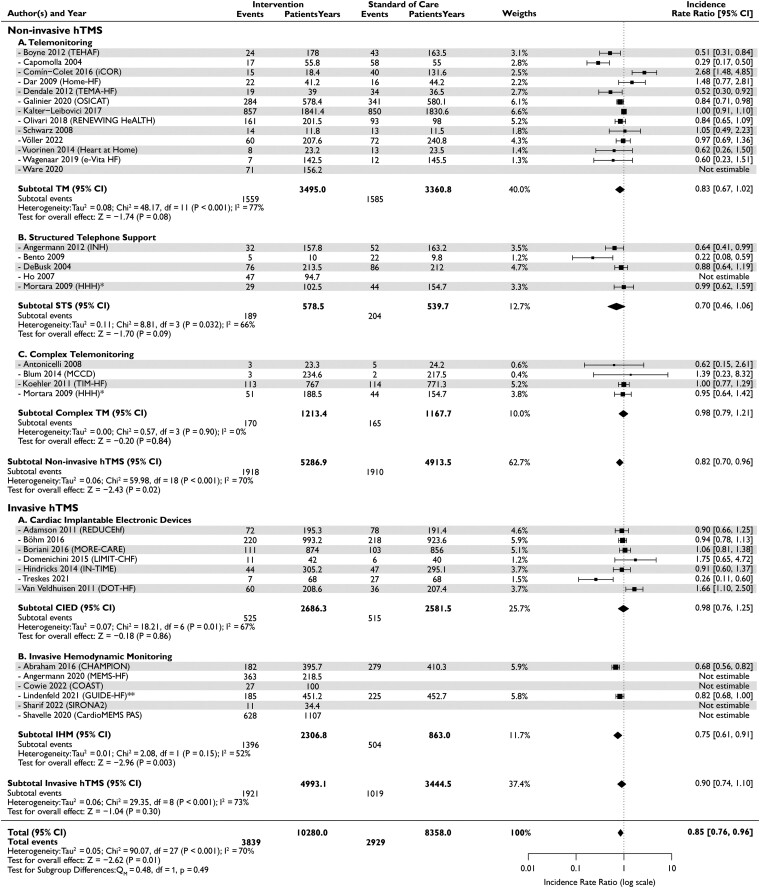
Methods and results: A systematic literature search was performed in four bibliographic databases, including randomized trials and observational studies that were published during January 1996-July 2022. A random-effects meta-analysis was carried out comparing hTMS with standard of care. All-cause mortality, first HF hospitalization, and total HF hospitalizations were evaluated as study endpoints. Sixty-five non-invasive hTMS studies and 27 invasive hTMS studies enrolled 36 549 HF patients, with a mean follow-up of 11.5 months. In patients using hTMS compared with standard of care, a significant 16% reduction in all-cause mortality was observed [pooled odds ratio (OR): 0.84, 95% confidence interval (CI): 0.77-0.93, I2: 24%], as well as a significant 19% reduction in first HF hospitalization (OR: 0.81, 95% CI 0.74-0.88, I2: 22%) and a 15% reduction in total HF hospitalizations (pooled incidence rate ratio: 0.85, 95% CI 0.76-0.96, I2: 70%).
Conclusion: These results are an advocacy for the use of hTMS in HF patients to reduce all-cause mortality and HF-related hospitalizations. Still, the methods of hTMS remain diverse, so future research should strive to standardize modes of effective hTMS.
Keywords: Heart failure; Hospitalization; Invasive; Mortality; Non-invasive; Telemonitoring.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: D.T. received research grants from Boston Scientific and Biotronik. O.M. received consulting fees from Abbott, AstraZeneca, and Boehringer-Ingelheim. R.d.B. has received research grants and/or fees from AstraZeneca, Abbott, Boehringer-Ingelheim, Cardior Pharmaceuticals GmbH, Ionis Pharmaceuticals, Inc., Novo Nordisk, and Roche; and has had speaker engagements with Abbott, AstraZeneca, Bayer, Bristol Myers Squibb, Novartis, and Roche. R.v.d.B. received an independent research grant and speaker fee from Abbott. J.B. received independent research grant from Abbott for ISS and has had speaker engagement or advisory boards in the past 5 years with Astra Zeneca, Abbott, Boehringer-Ingelheim, Bayer, Daiichi Sankyo, Novartis and Vifor. All other authors declared to have no conflict of interest.
Figures


Comment in
-
Is telemonitoring for heart failure ready after a journey longer than two decades?Eur Heart J. 2023 Aug 14;44(31):2927-2929. doi: 10.1093/eurheartj/ehad395. Eur Heart J. 2023. PMID: 37366251 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
