

Vitamin K1 and progression of cardiovascular calcifications in hemodialysis patients: the VitaVasK randomized controlled trial
- PMID: 37216675
- PMCID: PMC9664584
- DOI: 10.1093/ckj/sfac184
Vitamin K1 and progression of cardiovascular calcifications in hemodialysis patients: the VitaVasK randomized controlled trial
Abstract
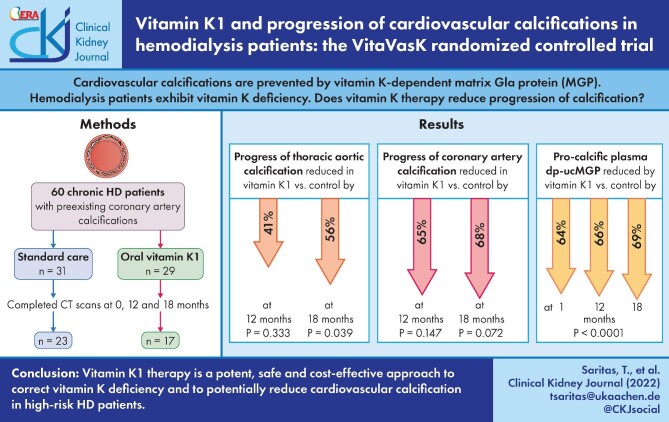
Background: Cardiovascular calcifications are prevented by matrix Gla protein (MGP), a vitamin K-dependent protein. Haemodialysis patients exhibit marked vitamin K deficiency. The randomized, prospective, open-label, multicentre VitaVasK trial analysed whether vitamin K1 supplementation reduces progression of coronary artery calcifications (CACs) and thoracic aortic calcifications (TACs).
Methods: Patients with pre-existing CACs were randomized to continue on standard care or to additionally receive 5 mg of vitamin K1 orally thrice weekly. Hierarchically ordered primary endpoints were progression of TAC and CAC in computed tomography scans at 18 months. Linear mixed effects models with repeated measures at baseline and 12 and 18 months assessed treatment effects after adjusting for study site.
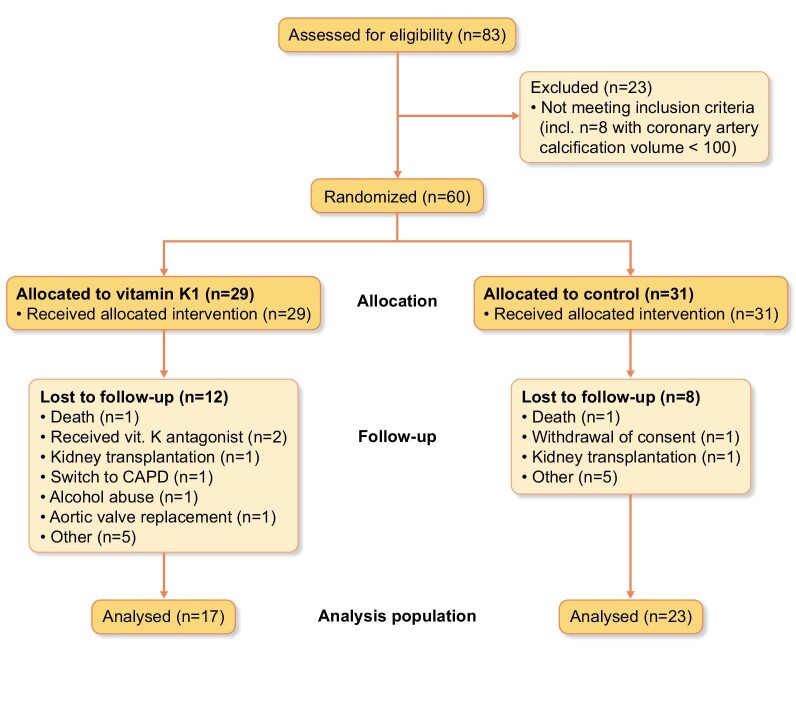
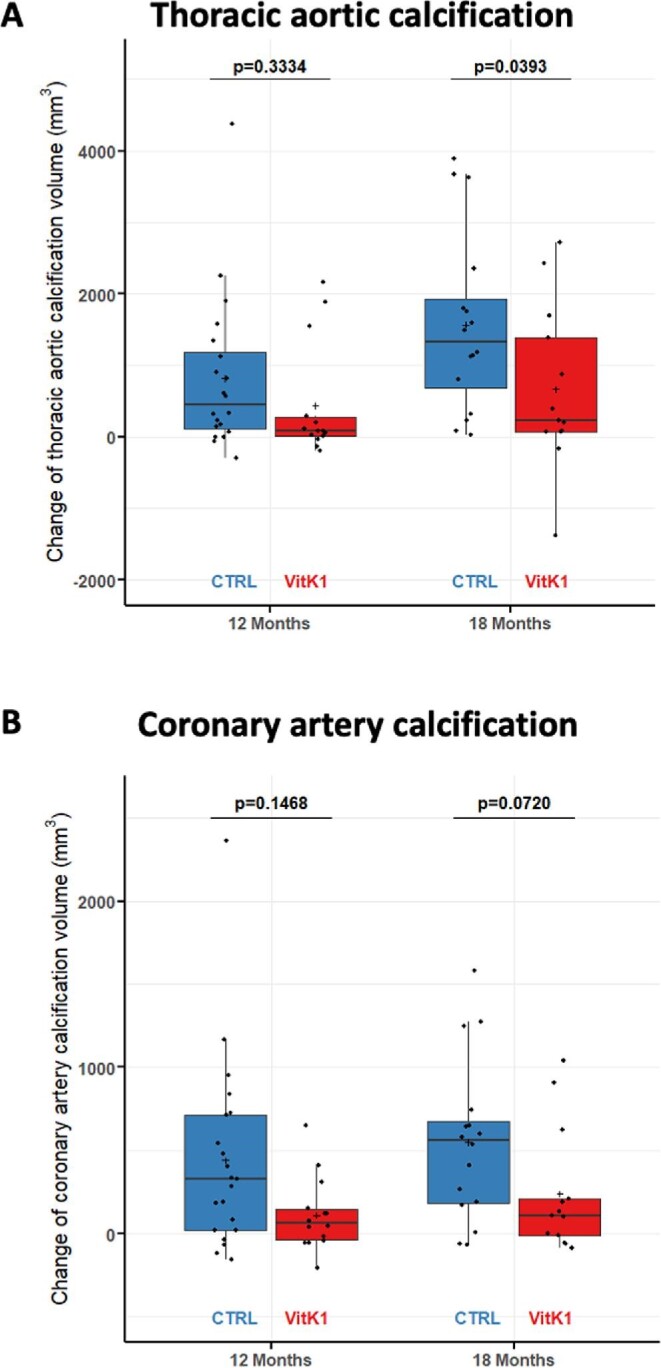
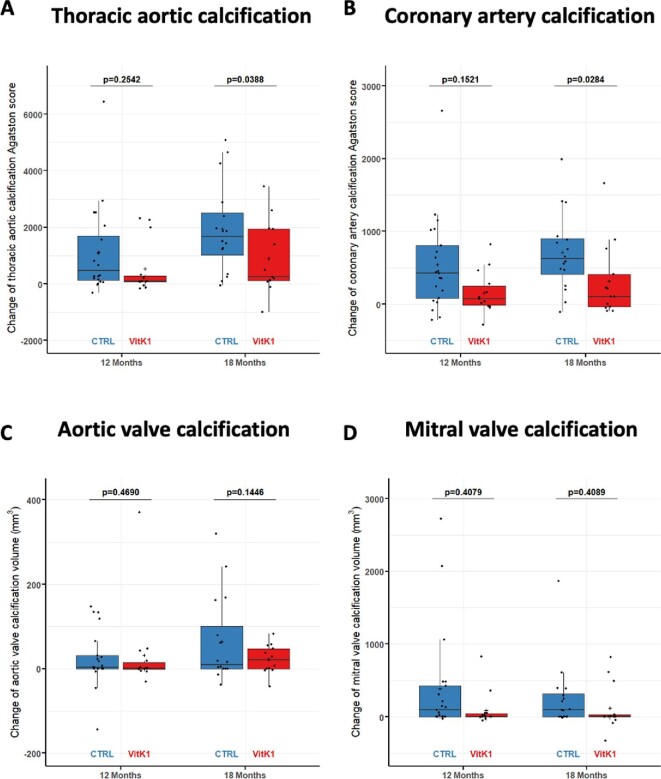
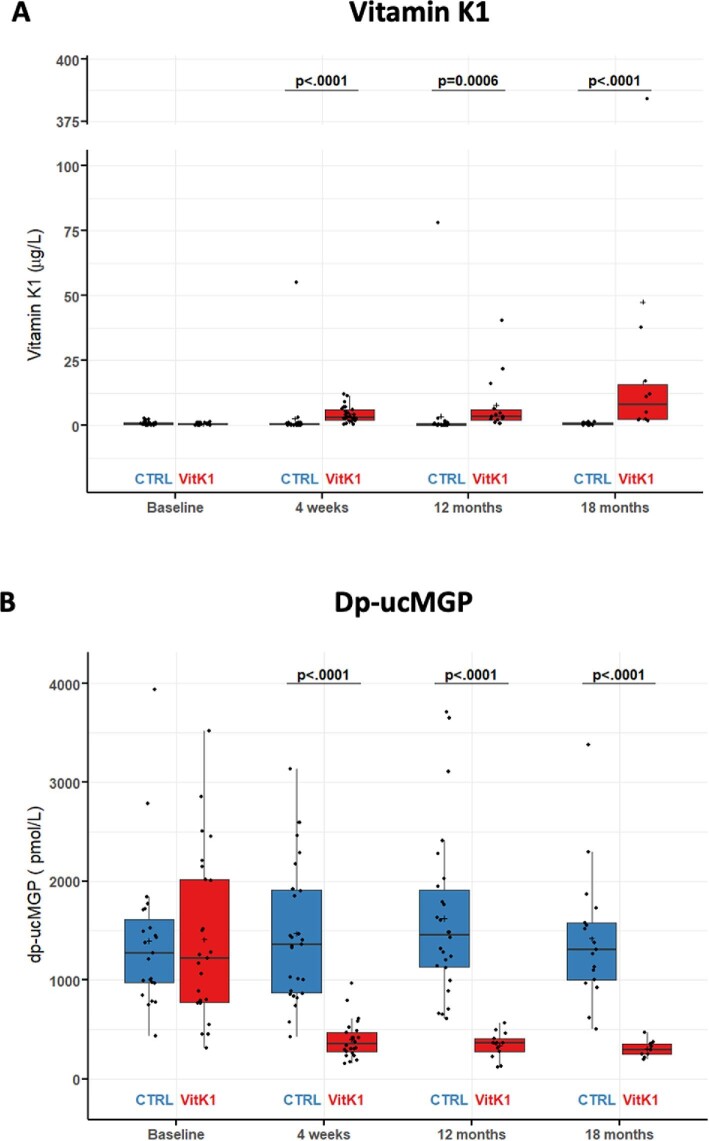
Results: Of 60 randomized patients, 20 dropped out for reasons unrelated to vitamin K1, resulting in 23 control and 17 vitamin K1 patients. The trial was stopped early due to slow recruitment. At 18 months, the average TAC progression was 56% lower in the vitamin K1 compared with the control group (p = .039). CAC significantly progressed within the control group, but not within the vitamin K1 group. Average progression at 18 months was 68% lower in the vitamin K1 compared to the control group (P = .072). Vitamin K1 reduced plasma levels of pro-calcific uncarboxylated MGP by 69% at 18 months. No treatment-related adverse events were noted.
Conclusion: Vitamin K1 intervention is a potent, safe and cost-effective approach to correct vitamin K deficiency and to potentially reduce cardiovascular calcification in this high-risk population.
Keywords: matrix Gla protein; valvular calcification; vascular calcification; vitamin K.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Tonelli M, Muntner P, Lloyd Aet al. . Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet 2012;380:807–14. - PubMed
-
- Schlieper G, Schurgers L, Brandenburg Vet al. . Vascular calcification in chronic kidney disease: an update. Nephrol Dial Transplant 2016;31:31–39. - PubMed
-
- Luo G, Ducy P, McKee MDet al. . Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature 1997;386:78–81. - PubMed
-
- Kaesler N, Schurgers LJ, Floege J.. Vitamin K and cardiovascular complications in CKD patients. Kidney Int 2021;100:1023–36. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
