

Crinecerfont, a CRF1 Receptor Antagonist, Lowers Adrenal Androgens in Adolescents With Congenital Adrenal Hyperplasia
- PMID: 37216921
- PMCID: PMC10583973
- DOI: 10.1210/clinem/dgad270
Crinecerfont, a CRF1 Receptor Antagonist, Lowers Adrenal Androgens in Adolescents With Congenital Adrenal Hyperplasia
Abstract
Context: Crinecerfont, a corticotropin-releasing factor type 1 receptor antagonist, has been shown to reduce elevated adrenal androgens and precursors in adults with congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency (21OHD), a rare autosomal recessive disorder characterized by cortisol deficiency and androgen excess due to elevated adrenocorticotropin.
Objective: To evaluate the safety, tolerability, and efficacy of crinecerfont in adolescents with 21OHD CAH.
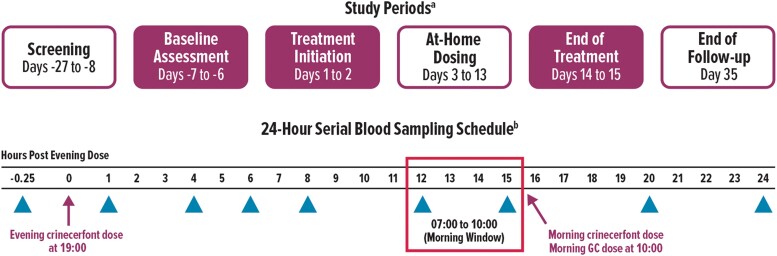
Methods: This was an open-label, phase 2 study (NCT04045145) at 4 centers in the United States. Participants were males and females, 14 to 17 years of age, with classic 21OHD CAH. Crinecerfont was administered orally (50 mg twice daily) for 14 consecutive days with morning and evening meals. The main outcomes were change from baseline to day 14 in circulating concentrations of ACTH, 17-hydroxyprogesterone (17OHP), androstenedione, and testosterone.
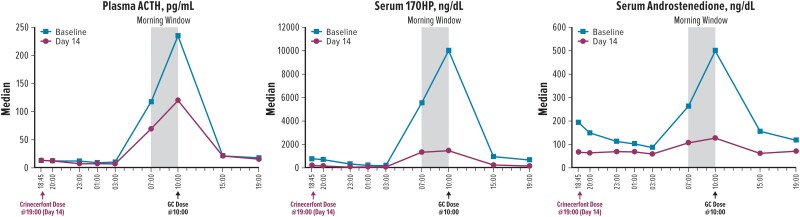
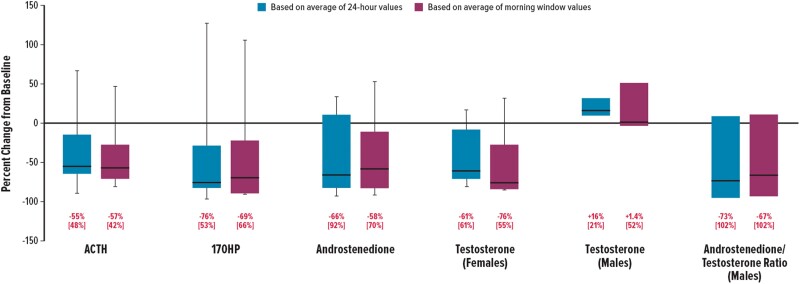
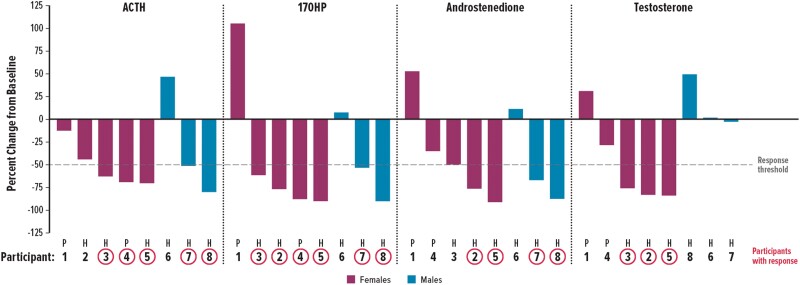
Results: 8 participants (3 males, 5 females) were enrolled; median age was 15 years and 88% were Caucasian/White. After 14 days of crinecerfont, median percent reductions from baseline to day 14 were as follows: ACTH, -57%; 17OHP, -69%; and androstenedione, -58%. In female participants, 60% (3/5) had ≥50% reduction from baseline in testosterone.
Conclusion: Adolescents with classic 21OHD CAH had substantial reductions in adrenal androgens and androgen precursors after 14 days of oral crinecerfont administration. These results are consistent with a study of crinecerfont in adults with classic 21OHD CAH.
Keywords: 21-hydroxylase deficiency; CRF type 1 receptor antagonist; adolescents; congenital adrenal hyperplasia; crinecerfont; pediatric.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Crinecerfont in a First Clinical Application of a CRH Antagonist: Further Potential Uses Are Still an Open Chapter!J Clin Endocrinol Metab. 2024 Mar 15;109(4):e1365-e1366. doi: 10.1210/clinem/dgad513. J Clin Endocrinol Metab. 2024. PMID: 37650613 No abstract available.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
