

Implementation of the YEARS algorithm to optimise pulmonary embolism diagnostic workup in the emergency department
- PMID: 37217241
- PMCID: PMC10231008
- DOI: 10.1136/bmjoq-2022-002119
Implementation of the YEARS algorithm to optimise pulmonary embolism diagnostic workup in the emergency department
Abstract
Background: Excessive use of CT pulmonary angiography (CTPA) to investigate pulmonary embolism (PE) in the emergency department (ED) contributes to adverse patient outcomes. Non-invasive D-dimer testing, in the context of a clinical algorithm, may help decrease unnecessary imaging but this has not been widely implemented in Canadian EDs.
Aim: To improve the diagnostic yield of CTPA for PE by 5% (absolute) within 12 months of implementing the YEARS algorithm.
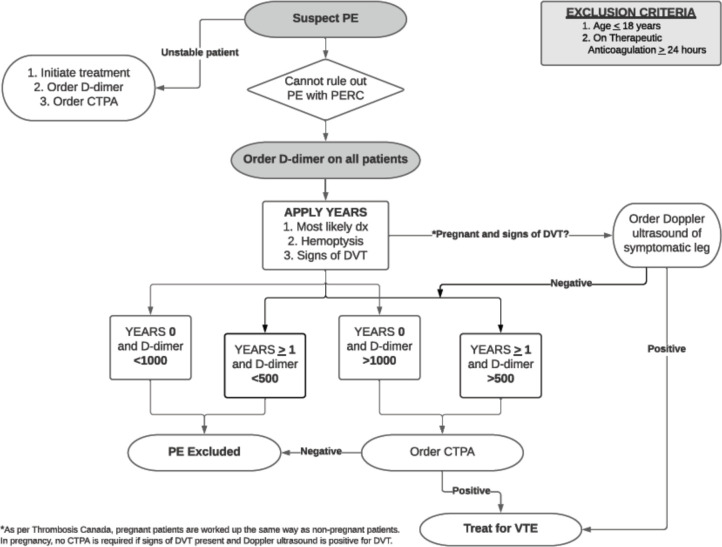
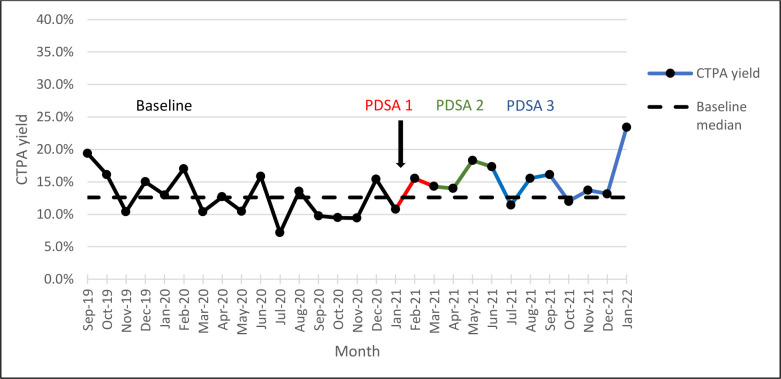
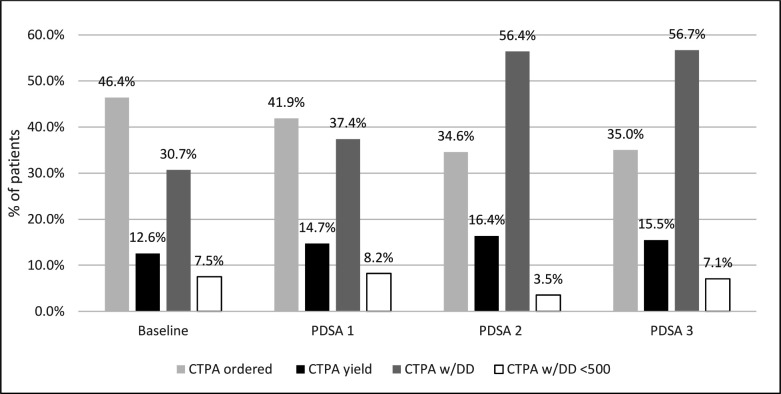
Measures and design: Single centre study of all ED patients >18 years investigated for PE with D-dimer and/or CTPA between February 2021 and January 2022. Primary and secondary outcomes were the diagnostic yield of CTPA and frequency of CTPA ordered compared with baseline. Process measures included the percentage of D-dimer tests ordered with CTPA and CTPAs ordered with D-dimers <500 µg/L Fibrinogen Equivalent Units (FEU). The balancing measure was the number of PEs identified on CTPA within 30 days of index visit. Multidisciplinary stakeholders developed plan- do-study-act cycles based on the YEARS algorithm.
Results: Over 12 months, 2695 patients were investigated for PE, of which 942 had a CTPA. Compared with baseline, the CTPA yield increased by 2.9% (12.6% vs 15.5%, 95% CI -0.06% to 5.9%) and the proportion of patients that underwent CTPA decreased by 11.4% (46.4% vs 35%, 95% CI -14.1% to -8.8%). The percentage of CTPAs ordered with a D-dimer increased by 26.3% (30.7% vs 57%, 95% CI 22.2% 30.3%) and there were two missed PE (2/2695, 0.07%).
Impact: Implementing the YEARS criteria may safely improve the diagnostic yield of CTPAs and reduce the number of CTPAs completed without an associated increase in missed clinically significant PEs. This project provides a model for optimising the use of CTPA in the ED.
Keywords: Clinical Decision-Making; Emergency department; Venous Thromboembolism.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Utilization of serum D-dimer assays prior to computed tomography pulmonary angiography scans in the diagnosis of pulmonary embolism among emergency department physicians: a retrospective observational study.BMC Emerg Med. 2021 Jan 19;21(1):10. doi: 10.1186/s12873-021-00401-x. BMC Emerg Med. 2021. PMID: 33468044 Free PMC article.
-
Over-Testing for Suspected Pulmonary Embolism in American Emergency Departments: The Continuing Epidemic.Circ Cardiovasc Qual Outcomes. 2020 Jan;13(1):e005753. doi: 10.1161/CIRCOUTCOMES.119.005753. Epub 2020 Jan 20. Circ Cardiovasc Qual Outcomes. 2020. PMID: 31957477
-
Use of YEARS Algorithm in Military Health Care Beneficiaries to Evaluate Use of Computed Tomography Pulmonary Angiography.Mil Med. 2023 Jul 22;188(7-8):e2380-e2386. doi: 10.1093/milmed/usac332. Mil Med. 2023. PMID: 36350772
-
Pulmonary embolism prevalence among emergency department cohorts: A systematic review and meta-analysis by country of study.J Thromb Haemost. 2021 Jan;19(1):173-185. doi: 10.1111/jth.15124. Epub 2020 Nov 18. J Thromb Haemost. 2021. PMID: 33048461
-
Diagnostic Blood Biomarkers for Acute Pulmonary Embolism: A Systematic Review.Diagnostics (Basel). 2023 Jul 6;13(13):2301. doi: 10.3390/diagnostics13132301. Diagnostics (Basel). 2023. PMID: 37443693 Free PMC article. Review.
Cited by
-
Implementation of an electronic ordering algorithm based on the YEARS criteria to optimize pulmonary embolism diagnostic workup in the emergency department.CJEM. 2025 Feb;27(2):123-128. doi: 10.1007/s43678-024-00840-y. Epub 2025 Feb 11. CJEM. 2025. PMID: 39932659
-
Type of D-dimer assay determines the diagnostic yield of computed tomography in patients suspected for pulmonary embolism.Res Pract Thromb Haemost. 2024 Nov 29;9(1):102638. doi: 10.1016/j.rpth.2024.102638. eCollection 2025 Jan. Res Pract Thromb Haemost. 2024. PMID: 39810983 Free PMC article.
-
Pulmonary artery choriocarcinoma mimicking pulmonary thromboembolism: a case report.Transl Cancer Res. 2024 Dec 31;13(12):7026-7037. doi: 10.21037/tcr-2024-2461. Epub 2024 Dec 27. Transl Cancer Res. 2024. PMID: 39816550 Free PMC article.
-
D-dimer diagnostics: can I use any D-dimer assay? Bridging the knowledge-to-action gap.Res Pract Thromb Haemost. 2024 Feb 1;8(1):102335. doi: 10.1016/j.rpth.2024.102335. eCollection 2024 Jan. Res Pract Thromb Haemost. 2024. PMID: 38433976 Free PMC article.
-
A review of the use of CT pulmonary angiography in pregnant and postpartum women at an academic centre.Obstet Med. 2024 Oct 26:1753495X241290551. doi: 10.1177/1753495X241290551. Online ahead of print. Obstet Med. 2024. PMID: 39553164 Free PMC article.
References
-
- Thrombosis Canada . Pulmonary embolism (PE): diagnosis. Available: https://thrombosiscanada.ca/clinicalguides [Accessed 22 May 2022].
MeSH terms
LinkOut - more resources
Full Text Sources
Medical